Download
1 / 147
1.58k likes | 2.45k Views
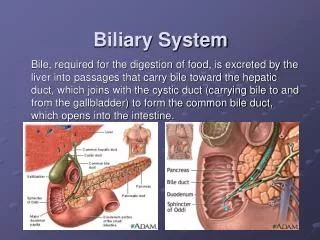
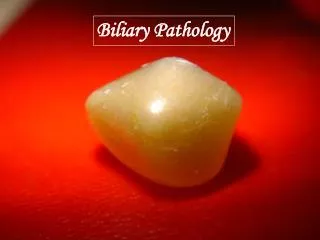
Biliary system. Anatomy. Plain x ray. GB stone in 10 %. Gas in biliary tree. Gall stone ileus. Gas in GB wall. Porcilin GB. Radiological investigations Oral Cholecystography. We comment on Site Size Shape Filling Defect Function Concentration of dye contractility. Investigations.

E N D
Plain x ray GB stone in 10 % Gas in biliary tree Gall stone ileus Gas in GB wall Porcilin GB
Radiological investigationsOral Cholecystography • We comment on • Site • Size • Shape • Filling Defect • Function • Concentration of dye • contractility
Investigations Imaging techniques Ultrasound this is most useful • Most important to show intrahepatic bile ducts dilatation • Measure the diameter of CBD (normal up to 7 mm) • Comment on the status of the GB and its stones • Visualize CBD diameter, stones or areas of narrowing • Tumors in the region of the pancreas is seen CT (conventional or helical) competes with the U/S especially as regards the pancreatic tumors.
cholangiogram • Preoperative cholangiogram • IV cholangiogram • PTC • ERCP • Intra operative • T tube ( post operative )
Investigations for a case of obstructive jaundice ERCP • ERCP is an outpatient procedure that combines endoscopic and radiologic modalities to visualize both the biliary and pancreatic duct systems. • Endoscopically, the ampulla of Vater is identified and cannulated. • A contrast agent is injected into these ducts, and • x-ray images are taken to evaluate their caliber, length, and course. • ERCP is used to • get a final diagnosis and • do biopsy of ampullary tumors, or brush cytology.
Investigations for a case of obstructive jaundice ERCP • It can be also therapeutic for • stone extraction by Dormia basket or • insertion of a stent, both are preceded by sphincterotomy. • It has its risks • ascending infections, • perforations, • pancreatitis, an • bleeding due to sphincterotomy done routinely before CBD cannulation
Congenitalcaroli’s syndrome congenital intrahepatic dilated bile ducts
Investigations for a case of obstructive jaundice MRCP • a sensitive noninvasive method of detecting biliary and pancreatic duct stones, strictures, or dilatations within the biliary system. • It is also sensitive for helping detect cancer.
Investigations for a case of obstructive jaundice MRCP (contraindications) Absolute include • the presence of a cardiac pacemaker, • cerebral aneurysm clips, • ocular or cochlear implants • ocular foreign bodies. Relative contraindications include • the presence of cardiac prosthetic valves, • neurostimulators, • metal prostheses, • penile implants
Investigations for a case of obstructive jaundice PTC • performed by a radiologist using fluoroscopic guidance. • The liver is punctured to enter the peripheral intrahepatic bile duct system. • An iodine-based contrast medium is injected into the biliary system and flows through the ducts. • Obstruction can be identified on the fluoroscopic monitor.
Investigations for a case of obstructive jaundice PTC • It is especially useful for lesions proximal to the common hepatic duct. • Still, ERCP is generally preferred. • PTC is reserved for use if ERCP fails or when altered anatomy precludes accessing the ampulla.
Investigations for a case of obstructive jaundice PTC Complications of this procedure include • the possibility of allergic reaction to the contrast medium. • peritonitis. • intraperitoneal hemorrhage, sepsis • cholangitis. • subphrenic abscess. • lung collapse. • Severe complications occur in 3% of cases
Investigations for a case of obstructive jaundice • Endoscopic ultrasound (EUS) combines endoscopy and US to provide remarkably detailed images of the pancreas and biliary tree. • It uses higher-frequency ultrasonic waves compared to traditional US (3.5 MHz vs 20 MHz) • allows diagnostic tissue sampling via EUS-guided fine-needle aspiration (EUS-FNA).
Acute Cholecystitis • Acute obstructive (Calcular) • Acute Acalcaus • Acute emphysematous
Acute obstructive (Calcular)(Pathology) • Calcular obstruction • GB become hyperemic, oedematous & distended • Chemical inflammation • Release of Phosphlipases • Act on lecithin which is a mucosal protector transforming it into • Lysolecithin (mucosal toxin • Arachidonic acid (PG precursor) (inflammation) • Sepsis • Ecoli, klebsilla & strept which occur later on
Acute obstructive (Calcular)(Pathology) • Following acute inflammation the condition end by one of the following • Resolution • Mucocele • Empyema • Gangrene And perforation • Bilo-enteric fistula
Acute Acalcular Cholecystitis • It form 8 % • Risk factors are • Sepsis • Starvation • Prolonged TPN • Ileus • Morphine use > 6 days
Acute Acalcular Cholecystitis • Pathology is not knowen • Prolonged distention of GB , Bile stasis & inspissations lead to mucosal injury and vessel thrombosis • Hypersensitivity to concomitant antibiotics • Gangrene occur in 25 % of cases
Acute emphysematous GB • Caused by mixed poly-microbial infection including gas forming bacteria • 70% male , diabetics • Thrombosis of cystic artery is the cause • It lead tom • Gangrene in 75 % • Perforation in 15 %
Clinical picture • Patient 5 F • General • High fever with shivering • Nausea, vomiting & biliary dyspepsia • Local • Biliary colic • Tenderness • Murphy’s sign • Boa’s sign • Complication
Clinical picture • The attack of biliary colic is the start with visceral type of pain (diffuse, colicky, radiating, and associated with vomiting) • Later on after 6 to 8 hours, the pain localizes to the right hypochondrium, and become associated with tenderness, rebound T, and rigidity and mild fever (somatic pain) • The presence of distended gall bladder is the hallmark of the disease, either discovered clinically or by U/S • In 25% of cases the bilirubin rises, due to compression of the CBD (Mirrizi syndrome) or less commonly due to an associated stone CBD • Serum amylase should be a routine as well as plain X ray abdomen (pancreatitis, and perforation or gas in biliary system