Download
1 / 42
431 likes | 739 Views
BILIARY MALIGNANCIES. Dr Sanjay De Bakshi MS(Cal.);FRCS (Eng Edin.). GALL BLADDER CANCER -Incidence. States of Uttar Pradesh, Bihar, West Bengal & Assam Delhi Madhya Pradesh; Bhopal have the highest incidence of Gall Bladder Cancer. AETIOLOGY.

E N D
BILIARY MALIGNANCIES Dr Sanjay De Bakshi MS(Cal.);FRCS (Eng Edin.).
GALL BLADDER CANCER-Incidence. • States of • Uttar Pradesh, • Bihar, • West Bengal & • Assam • Delhi • Madhya Pradesh; Bhopal • have the highest incidence of • Gall Bladder • Cancer.
AETIOLOGY • Cholelithiasis-directly proportional to the size of the stone;(Risk 2.4 for those with stones 2.0 to 2.9cm. in size; 10.1 for those with stones >3cm.) Metaplasia Dysplasia Carcinoma. • Papillary and non-papillary adenomas have pre-malignant potential, (in particular polyps >10mm in size). • Carcinogens-breakdown products from bile acids. • Anomalous connection between the CBD and Pancreatic ducts. • Porcelain Gall Bladder pathological finding of a brittle gallbladder with a bluish tinge. Diffuse (Type I)less prone than Selective mucosal calcification (Type II and III) Stephen et al 2001
AETIOLOGY • Occupational – possibly in the rubber industry. • Mustard oil loaded with impurities (Hai et al 1994). • Infections – Salmonella typhi, Helicobacter bilis and hepaticus and Esch. Coli implicated though the proof of relationship nebulous (Nath et al 2010) {Chronic inflammation and genotoxic toxin (cytotoxic distending toxin- CdtB)} PATHOBIOLOGY OF GALLBLADDER CANCER. Sunita Singh et al Journal of Scientific Research; Banaras Hindu University, Varanasi; Vol. 56, 2012 : 35-45
RISK FACTORS • Race • Obesity • Multiparity • Smoking • Chronic infections with S typhi and paratyphi • Porcelain Gall Bladder • Certain diet patterns.
STAGING OF GALL BLADDER CANCER Nevin et al 1976.
STAGING OF GALL BLADDER CANCER Donohue modification of Nevin classification 1990
STAGING OF GALL BLADDER CANCER AJCC/TMN 6th Edition
STAGING OF GALL BLADDER CANCER M N 0 No lymph node involvement 0 No distant mets AJCC/TMN 6th Edition 1 Distant mets incl. interaortocaval nodes 1 Any lymph node involvement
N STAGING7TH Edition M STAGING7TH Edition
Characteristics of a Gall Bladder Cancer • Spread principally by direct extension. • Spreads also by lymphatic, vascular,neural, intraperitoneal and intraductal routes. • Anatomically straddles the junction between the IVB and V lobe of the liver.
Lymphatic drainage of the Gall Bladder • Cholecysto-retropancreatic • Cholecysto-coeliac. • Cholecysto-mesenteric
Presentation of Gall Bladder Carcinoma. • Histological surprise • Lump abdomen without jaundice. • Lump abdomen with jaundice. • From secondaries.
OLDER TRADITIONAL VIEW. Nevin Stage I or II, cured by cholecystectomy ALONE. RECENT VIEWS- Tumours with Tis and T1a staging with clear resection margin, no further treatment needed. For patients with T2 or advanced GB cancer, a completion second radical operation is only chance of cure. Histological Surprise- what to do? VERSUS
Histological Surprise- what to do? EARLY RE-EXLORATION BUT AFTER FOUR STEPS • Pathology reviewed regarding staging and status of cystic duct. • Staging with adequate preoperative imaging. • Assessment for fitness for another major surgery. • Counselling of patient and family.
Patient presents with a lump-without jaundice,- what to do? ? • NEED TO RULE OUT SPREAD TO • N2 NODAL COMPARTMENT AND • TO PERITONEUM
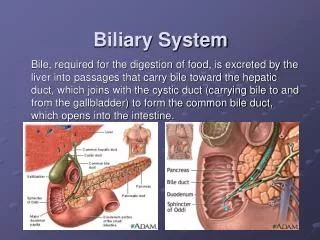
BILE DUCT CANCERAetiology • Prolonged cholestasis, inflammation and infection. • Choledochal cyst, Caroli’s disease, Congenital hepatic fibrosis and Polycystic disease. • After choledocho-enteric anastomosis and other previous biliary surgery(In the Lahey clinic series-50% had had cholecystectomy and 25% other types of biliary surgery.)
PERIPHERAL CHOLANGIOCAs • In most peripheral cholangiocarcinomas, hard, compact, and grayish-white massive or nodular lesions are found in the liver. • PET Sensitive.
BILE DUCT CANCERAetiology • Infection with liver flukes(Round worms?) • Chronic typhoid carrier states(x6 times) • Ulcerative colitis. • Solitary adenomas & biliary papillomas.
Pathology of the Bile Duct Cancer • TYPE-almost always adenocarcinomas • Sclerosing-70%. • Papillary-20%. • Nodular-10%. • SITE:- %
THE PROBLEM OF STAGING SYSYTEMS FOR BILE DUCT CARCINOMA • NONE ASSESS FOR RESECTABILITY • Most large series (for hilar tumours)- • 32% unresectable • 29% found to have secondaries at exploration • Therefore, a staging system has been proposed. • Based on Staging Laparoscopy (with Ultrasound). Janargin WR et al 2001
HILAR CARCINOMAS Janargin WR et al 2001
HILAR CARCINOMAS CRITERIA FOR NONRESECTABILITY • PATIENT FACTOR • Medically unfit • Cirrhosis/portal hypertension • LOCAL FACTORS • Hepatic duct involvement upto secondary radicles bilaterally • Encasement/occlusionof main portal vein proximal to its bifurcation • Atrophy of one lobe with encasement of contralateral portal vein branch • Atrophy of one lobe with contralateral secondary biliaryradicles involved • DISTANT DISEASE • Metastases to lymph node groups beyond hepatoduodenal ligament(Coeliac, Paraaortic, Retroduodenal – histo +ve) • Liver lung or peritoneum – histo +ve) Janargin WR et al 2001
DISTAL TUMOURS • Usually needs pancreatico-duodenectomy - • Longitudinal spread (less than pancreatic tumours) • True mid CBD tumours difficult to define • Lymph node status only independent predictor of long time survival.
INTRAHEPATIC (PERIPHERAL) DUCTAL TUMOURS • Often a diagnosis of exclusion. • Liver mass, cytologically an adenocarcinoma and extensive search for primaries – unrewarding. (Nakanuma et al 1985) (Ohashi et al 1994) (Yamamoto et al 1998)
Bile Duct Cancer -What to do? FROZEN-SECTION OF DUCT ENDS A MUST TO EXCLUDE LONGITUDINAL SPREAD.
THANK YOU ACCESS THE PRESENTATION AT www.drsanjaydebakshi.org