Download
1 / 52
570 likes | 945 Views
Central Sleep Apnea Syndromes. 6 th Annual Conference Northwest Ohio Southeast Michigan Sleep Society May 1, 2009 Navin K Jain, MD. CENTRAL SLEEP APNEA “ period of at least 10 seconds without airflow, during which no ventilatory effort is evident”. Normal Control of Breathing.

E N D
Central Sleep Apnea Syndromes 6th Annual Conference Northwest Ohio Southeast Michigan Sleep Society May 1, 2009 Navin K Jain, MD
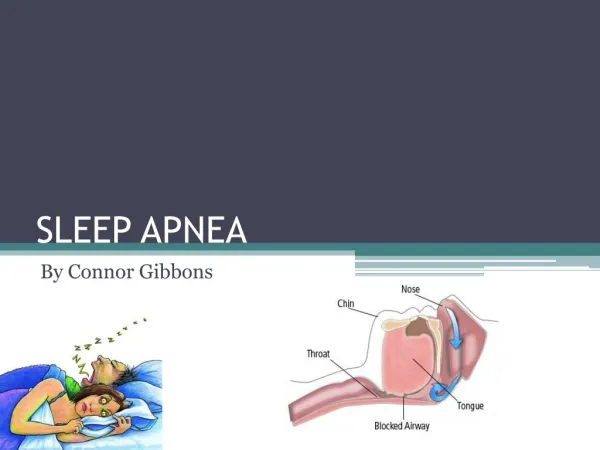
CENTRAL SLEEP APNEA “ period of at least 10 seconds without airflow, during which no ventilatory effort is evident”
Normal Control of Breathing • Automatic / Metabolic • Chemoreceptors (carotid body for hypoxia and carotid body and medullary receptors for hypercapnia and H ion) • Intrapulmonary receptors – vagus mediated • Brainstem processes • Keep ventilation regular and match to metabolic demands • Afferent Information from chest wall and respiratory muscles • Behavioral / Volitional – under voluntary control • Wakefulness stimulus – increased ventilation in awake state (ventilation persist during wakefulness in absence of metabolic mechanisms)
Control of Breathing at Sleep/Wake • Transition to Sleep • Loss of wakefulness stimulus and behavioral influences • Muscle activity and chemoreceptor sensitivity is reduced • Apnea threshold • Stable sleep changes – sleep specific CO2 set point • Transition to Wake - important to restore gas exchange; may cause central apnea: • Arousal threshold • Ventilatory Response to arousal
Control Of Breathing in Sleep • Non REM Sleep • Metabolic Control – input from chemoreceptors and vagal intrapulmonary receptors (oxygen administration in hypoxic individuals reduces ventilation and may prolong apneas in some individuals; hypocapnic alkalosis also reduces ventilation) • Response of chemoreceptors are somewhat reduced in Non REM sleep but still well maintained and maintains rhythmic ventilation during sleep • REM Sleep – further reduction in responsiveness of chemoreceptors
Central Sleep Apnea • Lack of drive to breathe during sleep • Lack of respiratory efforts during cessation of airflow • Insufficient or absent ventilation leading to compromised gas exchange • May lead to frequent nighttime awakenings leading to excessive daytime sleepiness and increased risk of adverse CV outcomes • Most patients have overlap of OSA and CSA • CSA Syndrome is considered primary diagnosis when >50% of apneas are scored as central in origin
CSA: Classification • Central Sleep Apnea • High Altitude Periodic Breathing • Idiopathic CSA • Narcotic Induced Central Apnea • Cheyne Stokes Breathing (CSB) • Obesity Hypoventilation Syndrome (OHS) (Hypercapneic CSA) • Complex Sleep Apnea
CSA Syndrome • Hypercapnic – impaired ventilatory output during wakefulness (worsens is sleep as wakefulness stimulus is removed) • Impaired Central Drive • Impaired Respiratory Motor Control • Nonhypercapnic • Cheyne Stokes Breathing • Idiopathic CSA
Hypercapnic CSA: Impaired Central Drive • Lesions of brain stem – tumors, trauma induced lesions • Congenital Central Hypoventilation Syndrome (Ondine’s curse) • Long term use of Opioids – prolonged periods of hypoventilation with marked hypoxemia and repetitive central apneas; dose dependent effects • Obesity Hypoventilation Syndrome (OHS)
CSA: Neurologic causes • Disorders of autonomic system • Autonomic dysfunction - Shy Drager Syndrome • Familial Dysautonomia • Diabetes Mellitus • Damage to Brain Stem (respiratory centers) • Post Polio syndrome • Tumor, Infection, Hemorrhage, encephalitis • Interruption of Neural pathways from medullary respiratory centers to ventilatory muscles • Cervical cordotomy
Chronic Opioid use • Becoming more common for chronic pain (even non malignant disorders) • Most experts believe – respiratory tolerance develops and respiratory depression is absent or mild • During wakefulness, chronic respiratory acidosis is absent or mild • While sleeping, 30-90% patients will have sleep apnea (central or obstructive) – may contribute to mortality
Obesity Hypoventilation Syndrome • Obesity – BMI > 35 • Alveolar Hypoventilation (PaCO2 >45 mm Hg) while awake • Hypoventilation worsens during non-REM sleep and further during REM sleep • Other causes of hypoventilation have been ruled out • COPD, Interstitial Lung Disease • Chest Wall Disease – Kyphoscoliosis • Hypothyroidism • Heart failure • Diaphragm Paralysis
Hypercapnic CSA: Impaired Respiratory Motor Control • Neuromuscular Disorders • Myasthenia Gravis • ALS • Post Polio Syndrome • Myopathies • Chest wall syndromes • Kyphoscoliosis
Nonhypercapnic CSA • CSB • Idiopathic CSA
Cheyne-Stokes Breathing (CSB) • Cyclic crescendo-decrescendo respiratory effort and airflow during wakefulness and sleep, without upper airway obstruction
Idiopathic CSA • Do not show CSB / transition apnea with normocapnia • May occur as distinct events or repetitive cyclical pattern • Duration of cycle – usually 20-40 seconds; less severe O2 desaturations • Mainly in stage N1 and N2 sleep • Arousals at termination of apnea • May complain of insomnia or hypersomnia • Usually have elevated hypercapnic ventilatory response
High Altitude Periodic Breathing • Most healthy individuals will have periodic breathing on high altitude ascent provide ascent causes significant alveolar hypoxia
Factors affecting CSA severity • Hypoxia • Any hypoxia tends to worsen CSA severity • More severe hypoxia seen in OHS; mild in idiopathic CSA and OHS • Hypoxia may impair respiratory sensory feedback • Upper Airway Anatomy • Narrow upper airway can collapse in central apnea (as it depends on neuronal input) • Treatment of OSA with PAP may cause hypocapnia in patients and may cause treatment emergent CSA by causing hypercapnia (Complex Sleep Apnea)
Cheyne-Stokes Breathing (CSB) • Cyclic crescendo-decrescendo respiratory effort and airflow during wakefulness and sleep, without upper airway obstruction • If decrescendo effort is accompanied by apnea during sleep, it is a type of central sleep apnea syndrome • Mainly seen is stage N1 and N2 sleep • Cycle time – 60-90 seconds (longer than other forms of CSA); correlation with severity of HF • Arousal typically occurs mid cycle at peak of ventilatory effort • Most commonly seen in patients with CHF and LV systolic dysfunction • Often co-exist with OSA (together may be classified as Sleep Disordered Breathing)
CSB: Pathogenesis • Uncertain • Seen as series of events • Patients are hypocapnic to begin with, so to correct hypocapnia, respiratory center initiates an apnea; pCO2 begins to rise. • Duration from beginning of apnea until respiratory center detects increasing PaCO2 is prolonged due to increased circulatory time • When respiratory center terminates apnea, it is already hypercapnia • Hypercapnia causes hyperpnea which causes hypocapnia • NET EFFECT – oscillation of ventilation between apnea and hyperpnea • Elimination of hypocapnia with inhaled CO2, CPAP or O2 can attenuate CSB
Factors contributing to CSB • High ventilatory drive • Minimal difference between apnea threshold and sleeping eucapnic PaCO2 • Long circulation time • Impaired cerebrovascular reactivity to CO2 • Increase pulmonary capillary wedge pressure may stimulate J receptors in lung causing apnea and resultant hyperventilation
Sleep Disordered Breathing (SDB) in Heart Failure • SDB may be seen in ~50% all patients with heart failure and ~70% patients with heart failure who are referred to sleep laboratory • Can be seen among patients whose heart failure is optimally managed • CSB may be more common than OSA in patients with heart failure • CSB more common among men, elderly, atrial fibrillation, and hypocapnia • OSA more common among older individuals and increasing BMI
CSB: Effects • Intermittent hypoxia – increased sympathetic drive causing arhythmia and worsening of HF • Arousals – induce adrenergic surges • Impair systolic and diastolic function • Extremely negative intrapleural pressure with hyperpnea increase ventricular transmural wall stress and afterload • CSB in patients with heart failure is associated with higher cardiac mortality • Clinically • Poor sleep quality – sleepiness in daytime • Symptoms of worsening heart failure – dyspnea, edema • Paroxysmal nocturnal dyspnea (due to hyperpnea) • Nocturnal angina, recurrent arrhythmia
CSB : Treatment • Management of CHF • Supplemental Oxygen • Acetazolamide • Theophylline • Pacemaker • Heart Transplantation • PAP therapy
Chronic Opioid use : CSA / CompSA • While sleeping, 30-90% patients on chronic opioids will have sleep apnea (central or obstructive) – may contribute to mortality • Acute uses – case report Chest 2008 (nightly dose) • low AHI • high sleep efficiency • Disproportionate symptoms (excess daytime sleepiness
CSA in Chronic Opioid Users • Develop combination of obstructive and central apnea events (pathogenesis – unknown) • Central events mainly in Non REM sleep • With PAP therapy, on CPAP obstructive events may be corrected and central events persist • When compared to age, gender, and BMI matched controls, higher AHI is due to central events • Dose relationship noted with AHI and dose of opioid • Central Apnea events • Periods of apnea and hyperepnea (Biot’s respiration) • Breaths at end of apnea are abrupt and not gradual • Irregular; erratic pattern of respiratory rate and tidal volume
CSA in Chronic Opioid Users • Central Apnea events • Periods of apnea and hyperepnea (Biot’s respiration) • Breaths at end of apnea are abrupt and not gradual • Irregular; erratic pattern of respiratory rate and tidal volume
Narcotic Induced CSA: Treatment • Minimize dose of Narcotics • PAP therapy • CPAP – alone not effective • Usually require APSSV
Obesity Hypoventilation Syndrome • Obesity – BMI > 35 • Alveolar Hypoventilation (PaCO2 >45 mm Hg) • Hypoventilation worsens during non-REM sleep and further during REM sleep • Other causes of hypoventilation have been ruled out • COPD, Interstitial Lung Disease • Chest Wall Disease – Kyphoscoliosis • Hypothyroidism • Heart failure • Diaphragm Paralysis
OHS: clinical features • Symptoms similar to OSA • Loud snoring, periods of choking in sleep, excessive sleepiness in daytime, fatigue • Dyspnea on exertion • BMI >35 kg/m2 • May heave features of Right Heart Failure • Rales, hepatomegaly, edema • Hypercapnia – PaCO2>45 mm Hg during wakefulness • Hypoxic – PaO2 <70 mm Hg but have normal alveolar-arterial gradient if no associated heart or lung disease • Elevated hematocrit • EKG, ECHO – features of RVH, Pulmonary HTN • PFT – restrictive ventilatory defect • Often have coexisting OSA
OHS: Pathogenesis Obesity Related Physiologic abnormalities • OSA • Increased work of breathing – due to reduced lung compliance and increased effort to move ribs and diaphragm • Respiratory Muscle Impairment - • Depressed Central Ventilatory Drive – reduced response to chemostimuli – hypoxia and hypercapnia (it may be effect of OHS rather than cause) • V/Q mismatching – poor ventilation of lower lobes and increased perfusion to lower lobes • Diminished effects of neurohumoral modulators (leptin) due to reduce levels or resistance • Weight Loss alone can cause decrease in PaCO2 during wakefulness in these patients
OHS and sleep study • Oxygen desaturation during sleep • Occur for longer periods than in patients who have OSA alone • Most patients have associated OSA • AHI severity is not associated with likelihood of coexisting OHS but severe oxygen desaturation is associated with coexisting OHS
OHS: Treatment • Weight Loss • Respiratory Stimulants • Progesterone • PAP therapy • Oxygen • Phlebotomy
Treatment Emergent CSA Complex Sleep Apnea (CompSA)
Complex Sleep Apnea (CompSA) • Described by Morgenthaler; Sleep2006 29:1203-09 • Treatment emergent central sleep apnea • Persistence or emergence of central apneas or hypopneas upon exposure to CPAP or an E0470 device when obstructive events have disappeared • Controversial – is it really a disease
CompSA: A Disease • Patients have anatomic and physiologic vulnerability causing OSA and a central breathing control instability • Seen more among men • Less sleep maintenance insomnia complaint • Higher likelihood of CHF or ischemic heart disease • Is it transient or persist if treated with CPAP alone
CompSA: Not a Disease • Transient and disappear with CPAP therapy in most patients • Relief of upper airway obstruction may cause change in CO2 excretion (so PaCO2 falls below apnea threshold) • Over titration • Activation of lung stretch receptors inhibits central respiratory motor input • Washout of CO2 from anatomic dead space • Increased transitions from sleep to wake as getting used to PAP – CPAP initiation may worsen sleep quality
PAP therapy • Continuous PAP (CPAP) • Useful in OSA • Useful in CSA with systolic heart failure • Bi-level PAP (BPAP) • Bi-level PAP with timed mode (BPAP S/T) • Adaptive Pressure Support Servo Ventilation (APSSV) • Used in patients with CSA, treatment emergent CSA, CSB