Download
1 / 25
260 likes | 520 Views
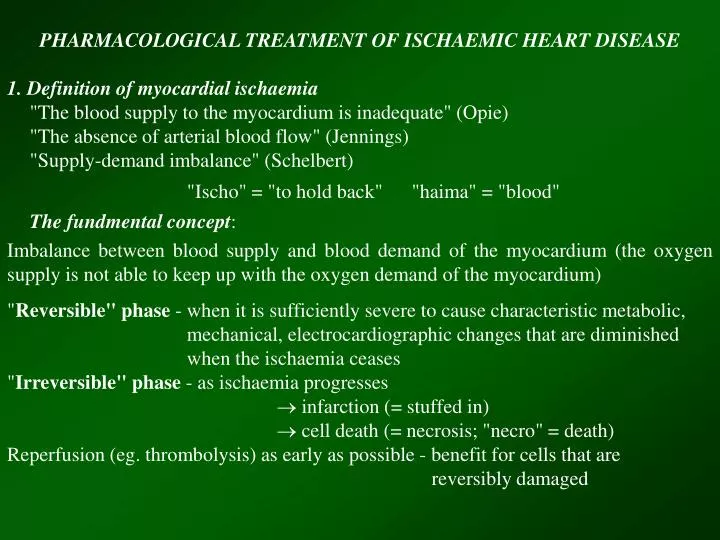
PHARMACOLOGICAL TREATMENT OF ISCHAEMIC HEART DISEASE 1. Definition of myocardial ischaemia "The blood supply to the myocardium is inadequate" (Opie) "The absence of arterial blood flow" (Jennings) "Supply-demand imbalance" (Schelbert) "Ischo" = "to hold back" "haima" = "blood"

E N D
PHARMACOLOGICAL TREATMENT OF ISCHAEMIC HEART DISEASE 1. Definition of myocardial ischaemia "The blood supply to the myocardium is inadequate" (Opie) "The absence of arterial blood flow" (Jennings) "Supply-demand imbalance" (Schelbert) "Ischo" = "to hold back" "haima" = "blood" The fundmental concept: Imbalance between blood supply and blood demand of the myocardium (the oxygen supply is not able to keep up with the oxygen demand of the myocardium) "Reversible" phase - when it is sufficiently severe to cause characteristic metabolic, mechanical, electrocardiographic changes that are diminished when the ischaemia ceases "Irreversible" phase - as ischaemia progresses infarction (= stuffed in) cell death (= necrosis; "necro" = death) Reperfusion (eg. thrombolysis) as early as possible - benefit for cells that are reversibly damaged
CAD (stenosis, spasm) Clinical manifestations Blood supply (oxygen supply) I. Conventional ischaemic syndromes - Angina pectoris - effort angina (classical) - angina at rest (vasospastic) - unstable angina - An myocardial infarction - Ischaemic cardiomyopathy II. New ischaemic syndromes - Silent ischaemia (1974) - Myocardial stunning (1975) (acute, chronic, maimed) - Hibernating myocardium (1984) - Ischaemic peconditioning (1986) Blood demand (oxygen demand) CHEST PAIN Impaired perfusion Metabolic changes aerobic anaerobic (lactate , inorganic P , H+, adenosine, ATP , CP , “osmotic load”) Impaired contractility “Litle blood, little work” Electrophysiological changes K+ ST-deviations, peaked T- Arrhythmias Exercise, emotional stress, exertion, increased sympathetic tone
PATHOPHYSIOLOGY OF ISCHAEMIC HEART DISEASE I. Conventional ischaemic syndromes 1.) Angina of effort (classic angina) •Coronary stenosis is the sine qua non of classical angina pectoris • Usually fixed coronary stenosis due to atherosclerosis (atherosclerotic plaques in the arterial trunks - morphologically, excentric or concentric). •Myocardium distal from a fix occlusion is potentially ischaemic (fall in CPP). Factors increase O2 demand (exercise, emotional stress, etc.), result coronary insufficiency (the fixed stenosis prevents coronary dilatation) and manifest clinically as myocardial ischaemia or anginal attack. 2.) Variant angina (angina at rest or vasospastic angina) • Vasospasm of coronary arteries (conductance vessels) may be responsible, which reduce CBF. Blood supply is inadequate even in resting heart. • Morphologic picture - normal or stenosed • Cyclic recurrent chest pain (ST-elevation), prolonged anginal attacks occur at the same time each day (eg. morning - "warm up" phenomenon), may culminate in myocardial infarction and sudden cardiac death. 3.) Unstable angina • Vasospasm superimposed upon more or less pronounced coronary stenosis. • Functional link between fixed stenosis (usually excentric) which restrict any increase in flow and the pure spasm (dynamic stenosis). • Mixed pathophysiological picture with changing intensity of the attacks (ST- elevation and depression), terminate usually in myocardial infarction.
4. Acute myocardial infarction Sudden and complete occlusion of a coronary artery. "No flow ischaemia". 5. Ischaemic cardiomyopathy II. New ischaemic syndromes 1. Silent ischaemia (1974; Stern and Tzivoni) • Episodes of silent ischaemia can cause temporary heart failure (reduced perfusion LV dysfunction). • The mechanism of silent ischaemia is poorly understood. Possible explanations may include an increased threshold for pain, and increased release of pain modifiers such as beta-endorphins. 2. Myocardial stunning 1975 Heyndrickx and colleagues (experimental), 1982 Braunwald and Kloner (clinical) A stunned myocardium is defined as viable myocardium salvaged by coronary reperfusion that exhibit prolonged postischaemic dysfunction after reperfusion. • Stunning can be characterised by delayed mechanical recovery despite full reperfusion after ischaemia „perfusion-contraction mismatch” • Acute stunning: mechanical function recovers minutes and hours • Chronic stunning: recovery is measured in weeks or months. • Maimed myocardium: incomplete recovery • Myocardial stunning may occur: in MI patients follwing thrombolysis or angioplasty, unstable angina patients, exercise-induced angina, coronary artery spasm, platelet aggregation or transient thrombosis of a coronary artery, angioplasty for chronic myocardial ischaemia, and immediately following coronary bypass surgery. • The concept is that ischaemia does something that impairs mechanical function or activity even after the actual ischaemic event is over.
3. Hibernating myocardium (1984 Rahimtoola) • Clinical observation: to describe a state of persistently impaired myocardial and left ventricular function at rest due to reduced coronary blood flow that can be partially or completely restored to normal if the myocardial oxygen supply-demand relationship is favourably altered either by improving blood flow and\or by reducing demand. •Hibernating myocardium is defined as ischaemic myocardium supplied by a narrowed coronary artery in which ischaemic cells remain viable but contraction is chronically depressed. •The current sine qua non concept for hibernating myocardium would be threefold: (1) impaired contractile activity (2) the presence of severe coronary artery disease (3) recovery of myocardial function after revascularisation •Hibernating myocardium is found in patients with severe coronary artery stenosis, even in asymptomatic patients at rest. 4. Mixed postinfarct ischaemic syndrome •This includes LV dysfunction and LV remodelling, postischaemic diastolic and systolic failure 5. Ischaemic preconditioning (1986; Murry, Jennnings, Reimer) • "Multiple brief ischaemic episodes might actually protect the myocardium during a subsequent sustained ischaemic insult, so that, in effect, we could exploit ischaemia to protect the heart from ischaemic injury"
Major determinants of myocardial oxygen supply and demand 1.) Factors influencing myocardial oxygen demand • Heart rate • Wall tension - preload and afterload • Myocardial contractility • Heart size 2.) Factors influencing myocardial oxygen supply • Hematologic factors - haemoglobin, free oxygen (pO2) • Myocardial extraction of oxygen from blood • Coronary blood flow (CBF) • coronary vascular resistance • autoregulation • compression of the deep arteries during diastole • fixed resistance (eg. atherosclerotic plaque) • coronary perfusion pressure (CPP) • distribution of the blood (endo/epi)
OBJECTIVE OF THE THERAPY 1.) Reduction of the frequency and severity of attacks of chest pain 2.) Remove of any underlying cause if possible 3.) Promotion of growth of collateral vessels 4.) Prevention of sudden cardiac death There are two ways to achieve these: 1. To improve coronary blood flow (?) 2. To reduce myocardial oxygen requirements - decrease preload - decrease afterload - decrease contractility - decrease heart rate - decrease sympathetic tone CLASSIC ANGINA VASOSPASTIC ANGINA UNSTABLE ANGINA NITRATES Ca++ ANTAGONISTS BLOCKERS
Drugs used in the treatment of angina pectoris -Blockers Calmodulin propranolol Ca2+ Calcium- antagonists Ca2+ - Ca2+ calmodulin complex Heart rate Contractility Oxygen demand nifedipine diltiazem verapamil + Systemic circulation Stored Ca2+ MLCKa MLCK Dilate Ca2+ -channels RELAXATION Dilate Arterial resistance vessels + Miosin light chain (MLC) MLC- MLC P Dilate Actin Nitrates gliceril-trinitrát izosorbide-dinitrate izosorbide-5- mononitrate cGMP GTP Dilate Tissue thiols Contraction Dilate REDUCED PRELOAD Guanilate- cyclase Venous capacitance vessels + RSNO RSH RSH Reduced venous return - NO3 NO - NO2 Reduced afterload Ischaemic area
BASIC PHARMACOLOGY OF VASODILATORS A: ORGANIC NITRITES AND NITRATES 1.) Chemistry Nitric and nitrous acid esters of polyalcohols (nitroglycerin = griceryl trinitrate) CH2 - O - NO2 CH - O - NO2 CH2 - O - NO2 All therapeutically active agents are capable of release nitric oxide (NO) in vascular smooth muscle cells. 2.) Pharmacological actions 2.1. Mechanism of action R - O - NO2 ENZYMATIC NON - ENZYMATIC R - O - NO2 cystein glutatione S transferase NO’ R - OH + NO2 NO3 guanylate cyclase NO2 NO3 cGMP GTP PROTEIN P KINASE PROTEIN KINASE PMLC MLC Ca++ CONTRACTION RELAXATION SMOOTH MUSCLE CELL
2.2. Organ system effects Nitroglycerin relaxes all types of smooth muscle resulting in general vasodilatation a.) Effects on coronary blood vessels • Dilates large coronary vessels (conductance vessels) but the total coronary blood flow is unchanged • Improves collateral circulation to the ischaemic area • Favoured perfusion to the subendocardium (explained by simple haemodynamic changes) b.) Effects on myocardial oxygen demand (1) Effects which reduce O2 demand • decreased preload (due to increased venous capacitance) • decreased afterload (due to reduced peripheral resistance) • decreased wall tension (decreased heart size and LVEDP/V) (2) Effects which increase O2 demand • increased heart rate (due to fall in blood pressure) • increased contractility (due to compensation) c.) Direct effect on the myocardium • niric oxide by stimulating guanylate cyclase increases cGMP • cGMP modulates L-type Ca2+ channels reduced Ca2+ influx • cGMP activates cGMP-dependent cAMP-phosphodiesterase, and results in a reduced Ca2+ influx Both effects reduce myocardial contractility and O2 consumption
NITROGLYCERIN 1. VENOUS DILATIION (pooling) extracardial PRELOAD factors {LVEDP, LVEDP, PCWP} O2 demand WALL TENSION endocardial perfusion 2. ARTERIAL DILATATION afterload CO 3. DILATATION OF LARGE intracardial CORONARY ARTERIES 02 supply factors 4. COLLATERAL CIRCULATION 3. Toxicity and tachyphylaxis Extension of therapeutic vasodilatation • orthostatic hypotension • tachycardia • throbbing headache Tolerance develops with continuous exposure (eg. chemical industry, explosives, Monday disease - headache, dizziness) Dependence: withdrawal symptoms - exacerbated myocardial ischaemia
4. Mechanism of clinical effect Potential beneficial effectsRESULTS Decreased ventricular volume Decreased arterial pressure Decreased myocardial Decreased ejection time oxygen requirements Vasodilation of epicardial Relief of coronary coronary arteries artery spasm Increased collateral flow Improved perfusion to the ischaemic area Decreased LVEDP Increased endocardial perfusion Potential deleterious effects Reflex tachycardia Increased myocardial Reflex increase in contractility oxygen requirements Decreased diastolic perfusion time Decreased myocardial due to tachycardia perfusion a.) Nitrate effects in angina of effort Reduced venous return reduces intracardiac volume reduces wall tension reduces O2 demand Decreased O2 demand during exercise is the primary effect (increased exercise tolerance) b.) Nitrate effects in angina at rest Vasodilatation of large epicardial coronary arteries relief of spasm c.) Nitrate effects in unstable angina Reduction of O2 demand + dilation of epicardial coronary arteries Relieve anginal attack and decrease the incidence of ischaemic episodes
5. Route of administration (1) To achieve an acute effect (to relief anginal pain) For this purpose: Sublingual or buccal tablets or spray - (rapid absorption) NITROGLYCERIN (Tabl. 0.5 mg) onset: 10-20 sec, duration 20 min ISOSORBIDE DINITRATE (ISORDIL) (Tabl. 2.5, 5 and 10 mg) AMYL NITRITE for inhalation, onset: 10 sec, duration 5-10 min Side effects: warmth, flushing, throbbing headache, dizziness, syncope, postural hypotension (2) For long term treatment (to prevent anginal attacks) For this purpose: oral tablets, transdermal patches, oinments - high degree of "first pass" hepatic biotransformation NITROGLYCERIN (NITRONG, SUSTAC) (Tabl: 0.5 mg), onset: 15 min, duration: several hours PENTAERYTHRYL TETRANITRATE, ERYTRYL TETRANITRATE, ISOSORBID MONONITRATE (ISMN), ISOSORBID DINITRATE (ISDN) NITRO-BID (NTG) for iv. infusion Topical administration - longer duration (6-24 h) NITRO-BID (2 % ointment) Transdermal patches: DEPONIT (NTG 5 mg/24h), NITRODUR (NTG 2.5 and 5 mg/24h) NITRODISC (NTG 5 mg/24h) MOLSIDOMINE New vasodilator with novel structure for oral administration. Improves exercise tolerance. No tachycardiac effect (less pronounced reduction in afterload)
6. Therapeutic uses Acute and chronic angina pectoris (stenotic, vasospastic), acute myocardial infarction, postinfarction angina, acute left ventricular failure (adjuvant therapy) B: CALCIUM ANTAGONISTS (CALCIUM CHANNEL BLOCKERS, SLOW CHANNEL BLOCKERS) 1.) Chemistry Different structures with similar actions a.) Monophenylalkilamines: VERAPAMIL, BENCYCLAN, PERHEXILIN b.) Diphenylalkilamines: FENDILINE, PRENYLAMINE, BEPRIDIL c.) Dihydropyridines: NIFEDIPINE, NISOLDIPINE, AMLODIPINE, FELODIPINE, NICARDIPINE, NITRENDIPINE d.) Benzothiazepine: DILTIAZEM e.) Diphenylpiperazines: FLUNARIZINE, CINARIZINE, LIDOFLAZIME
2.) Pharmacological actions All inhibit or block the influx of calcium through the voltage activated calcium channels. Voltage dependent calcium channels: • L-type (cardiac and vascular) • N-type (mostly neuronal) • T-type (neuronal and gland) Receptorial binding sites for nifedipine, diltiazem and verapamil are different. Voltage operated calcium channels open at -45 to -25 mV membrane potential inward calcium current (trigger calcium) promotes release of calcium from the sarcoplasmic reticulum (SR). (Na channels open at -90 to -50 mV, the Na+ inward current releases Ca2+ from the mithocondrium). Ca - ANTAGONIST RECEPTOR OPERATED VOLTAGE OPERATED Ca-pump + Ca2+ Ca2+ Ca2+ CALMODULIN ATP-ase Ca2+ - CALMODULIN COMPLEX cAMP regulates: Na+-K+-ATP-ase Ca2+ channel phosphorylation (PKC) Ca2+ influx SR Ca-ATPase Ca2+ sequestration into the SR Inactivation of MLCK Calcium-calmodulin complex formation cAMP + MLCK(a) MLCK(a) MLCK(PO4)2 (i) + } MYOSIN + ACTIN MYOSIN PO4 + ACTIN CONTRACTION MLCK = MYOSIN LIGHT CHAIN KINASE
3. Organ-system effects a.) SMOOTH MUSCLE - their contraction-relaxation is dependent upon Ca2+ influx. Calcium antagonists cause relaxation. Arterioles > veins reduction in peripheral vascular resistance. Arterial blood pressure reduces b.) CARDIAC MUSCLE - is highly dependent upon Ca2+ influx for normal function. • Impulse generation in SA node and impulse conduction through the AV node is based on slow inward current. Ca-blockers bradycardia and negative domotropic effect • Contractility of the myocardium is also depending on Ca2+ influx. Ca-blockers result in negative inotropic effect reduction in myocardial O2 demand (ATP preservation increases) reduction in ischaemic damage (infarct size) c.) SKELETAL MUSCLE - is not depressed by calcium antagonists (contraction not requires Ca influx, utilizes intracellular pools of calcium) COMPARISON OF CARDIOVASCULAR EFFECTS OF CALCIUM ANTAGONISTS 1. Reduction in coronary vascular resistance NIFEDIPINE >> DILTIAZEM > VERAPAMIL 2. Reduction in peripheral vascular resistance NIFEDIPINE >> VERAPAMIL > DILTIAZEM 3. Negative inotropic effect VERAPAMIL > DILTIAZEM >>>>> NIFEDIPINE 4. Depression of sinus node pacemaker DILTIAZEM > VERAPAMIL (NIFEDIPINE, reflex tachycardia) 5. Slowing of AV conduction VERAPAMIL > DILTIAZEM (NIFEDIPINE has no effect)
4. Side and toxic effects of calcium antagonists Direct extension of their therapeutic action Bradycardia, AV-block (especially verapamil), cardiac arrest, heart failure. Palpitation, reflex tachycardia, headache (especially after nifedipine) Flushing, edema, dizziness, nausea, constipation. 5. Mechanism of clinical effects Negative inotropic effect O2 requirements ANTIANGINAL EFFECT Vascular relaxation CORONARY ARTERIES • improved collateral flow infarct size • relief and prevention of coronary spasm Both result in ANTIANGINAL EFFECT PERIPHERAL ARTERIES • reduced vascular resistance (afterload and preload) ANTIANGINAL AND ANTIHYPERTENSIVE EFFECT Negative chronotropic (bradycardiac) effect Slowing HR O2 consumption improved myocardial perfusion during diastole) ANTIANGINAL AND ANTIARRHYTHMIC EFFECT Negative dromotropic effect Slowing conduction through the AV node ANTIARRHYTHMIC EFFECT
6. Clinical use of calcium antagonists (1) ANGINA PECTORIS (chronic stable angina, variant angina, unstable angina) VERAPAMIL, DILTIAZEM, NIFEDIPINE etc. Combinations with other antianginal drugs VERAPAMIL + BLOCKER (AV block and strong negative inotropy) NIFEDIPINE + BLOCKER (in HF patients, BUT in low pressure states NIFEDIPINE is contraindicated (2) HYPERTENSION - NIFEDIPINE, VERAPAMIL, DILTIAZEM (3) ATRIAL TACHYARRHYTHMIAS - WPW SYNDROME VERAPAMIL, DILTIAZEM 7. Drugs VERAPAMIL (ISOPTIN, CALAN) - antianginal, antiarrhythmic (Tabl.: 40, 80, 120 mg), ISOPTIN retard (better kinetic) NIFEDIPINE (ADALAT, PROCARDIA, CORINFAR) - vasospastic (Prinzmetal) and stable chronic angina, hypertension (Tabl. 10 mg) NITRENDIPINE and FELODIPINE hypertension NIMODIPINE profilactically after subaracnoid hemorrhage to prevent vasospasm DILTIAZEM (CARDIZEM, DILZEM) vasospastic and chronic stable angina (Tabl.: 30, 60, 90, 120 mg) FENDILINE (SENSIT) - calmodulin antagonist - antianginal, antihypertensive
C: BETA RECEPTOR BLOCKING DRUGS • They are not vasodilators. Their beneficial effects are related to the reduction in HR, blood pressure and contractility. These are all reduce myocardial oxygen requirements. • They result in redistribution of blood flow from the non-ischaemic to the ischaemic myocardial areas. • They decrease the episodes of anginal pain but not normalize ischaemic ST- depression. 1. Pharmacological actions a.) Effect on myocardial oxygen demand (1) Reduction in O2 demand (due to ß-rceptor antagonism) • decreased contractility • decreased heart rate (2) Increase in O2 demand (secondary to reduced contractility) • increased LVEDP (preload) • increased wall tension (due to increased heart size) These are undesirable effects. b.) Combination of ß-blockers with nitrates Aimed to offset each-other's deleterious effects on myocardial oxygen requirements NITRATES ß-BLOCKERS COMBINATION Heart rate reflex Blood pressure LVEDP 0/ TPR 0 Myocardial contractility reflex 0 LV ejection fraction variable Ejection time 0 Diastolic perfusion time
Individual titration: against both rest and exercise (HR monitoring with BP and cardiac function measurements). • HR at rest: 50-60 beats/min and during exercise: 100-120 beats/min • ß-blockers, however can precipitate heart failure (?) and bronchoconstriction may aggravate angina. 2. Drugs POPRANOLOL (INDERAL, ß1, ß2) METOPROLOL (LOPRESSOR, ß1) NADOLOL (ß1, ß2) ATENOLOL (TENORMIN, ß1) PINDOLOL (ß1, ß2, partial agonist) ACEBUTOLOL (ß1 partial agonist) ALPRENOLOL (ß1, ß2, partial agonist) TIMOLOL (ß1, ß2). GENERAL MANAGEMENT OF PATIENTS WITH ANGINA PECTORIS 1. Pharmacological 2. Surgical interventions AIM: Producing symptomatic relief and prolonging life PROGNOSTIC DETERMINANTS: • degree of LV dysfunction • event of coronary atherosclerosis • severity of myocardial ischaemia
High risk of AMI coronary arteriography severe multiple vessel disease bypass surgery Absence of high risk of AMI pharmacological treatment Immediate relief: NITRATES (sublingual, spray) Long term treatment: a.) Chronic stable angina: NITRATES + ß BLOCKERS (Ca ANTAGONISTS) b.) Unstable angina: immediate therapy - agressive NITRATE, ß-BLOCKER and Ca ANTAGONIST continuous manifestation revascularisation angioplasty c.) Variant angina: Ca ANTAGONISTS and NITRATES Patients with obstructive CAD ß-blockers may also be used In the presence of severe fixed obstructive coronary artery lesions, angioplasty and revascularisation.
Drugs used in the treatment of angina pectoris -Blockers Calmodulin propranolol Ca2+ Calcium- antagonists Reduced afterload Ca2+ - Ca2+ calmodulin complex Heart rate Contractility Oxygen demand nifedipine diltiazem verapamil + Systemic circulation Stored Ca2+ MLCKa MLCK Dilate Ca2+ -channels RELAXATION Dilate Arterial resistance vessels + Miosin light chain (MLC) MLC- MLC P Dilate Actin Nitrates gliceril-trinitrát izosorbide-dinitrate izosorbide-5- mononitrate cGMP GTP Dilate Tissue thiols Contraction Dilate REDUCED PRELOAD Guanilate- cyclase Ischaemic area Venous capacitance vessels + RSNO RSH RSH Reduced venous return - NO3 NO - NO2
Drugs used in the treatment of angina pectoris -Blockers Calmodulin propranolol Ca2+ Calcium- antagonists Ca2+ - Ca2+ calmodulin complex Heart rate Contractility Oxygen demand nifedipine diltiazem verapamil + Systemic circulation Stored Ca2+ MLCKa MLCK Dilate Ca2+ -channels RELAXATION Dilate Arterial resistance vessels + Miosin light chain (MLC) MLC- MLC P Dilate Actin Nitrates gliceril-trinitrát izosorbide-dinitrate izosorbide-5- mononitrate cGMP GTP Dilate Tissue thiols Contraction Dilate REDUCED PRELOAD Guanilate- cyclase Venous capacitance vessels + RSNO RSH RSH Reduced venous return - NO3 NO - NO2 Reduced afterload Ischaemic area
ORGANIC NITRITES AND NITRATES Route of administration (1) To achieve an acute effect (to relief anginal pain) For this purpose: Sublingual or buccal tablets or spray - (rapid absorption) NITROGLYCERIN (Tabl. 0.5 mg) onset: 10-20 sec, duration 20 min ISOSORBIDE DINITRATE (ISORDIL) (Tabl. 2.5, 5 and 10 mg) Side effects: warmth, flushing, throbbing headache, dizziness, syncope, postural hypotension (2) For long term treatment (to prevent anginal attacks) For this purpose: oral tablets, transdermal patches, oinments - high degree of "first pass" hepatic biotransformation NITROGLYCERIN (NITRONG, SUSTAC) (Tabl: 0.5 mg), onset: 15 min, duration: several hours PENTAERYTHRYL TETRANITRATE, ERYTRYL TETRANITRATE, ISOSORBID MONONITRATE (ISMN), ISOSORBID DINITRATE (ISDN) NITRO-BID (NTG) for iv. infusion Topical administration - longer duration (6-24 h) NITRO-BID (2 % ointment) Transdermal patches: DEPONIT (NTG 5 mg/24h), NITRODUR (NTG 2.5 and 5 mg/24h) NITRODISC (NTG 5 mg/24h)