Download
1 / 24
250 likes | 691 Views
The use of low arousal approaches to manage challenging behaviours in individuals with ASD:A conceptual framework. Andrew McDonnell, PhD. Clinical psychologist, Studio3 training Systems, Email: Andy@studio3.org. Autism is a heterogeneous construct.

E N D
Theuse of low arousal approaches to manage challenging behaviours in individuals with ASD:A conceptual framework Andrew McDonnell, PhD. Clinical psychologist, Studio3 training Systems, Email: Andy@studio3.org
Autism is a heterogeneous construct • It is important to stress the complexity of ASD. • There have been significant attempts to develop universal theories. • Too much research has focussed on falsifying various cognitive theories. • Some constructs may have an important mediating effects, especially, when considering challenging behaviours. • Arousal is not an unknown or new construct.
Arousal and autism • Physiological hyper arousal has been associated by researchers with childhood autism (Hutt, Hutt, Lee and Ounsted, 1964). • Sensory overeactivity has been explained as a possible response to overarousal (Liss, et al. 2006). • It has also been suggested that repetitive movements may serve a dearousing function (Kinsbourne, 1980).
Sensory issues • There is an increasing body of literature which identifies sensory issues. • ‘people have different thresholds for noticing, responding to and becoming irritated with sensations; reflected in their mood, temperament and ways of organising their lives’ (Dunn, 2001, p609)
Sensory issues • In a survey of UK parents of 75 children with ASD 71% appeared to be hypersensitive to sound, touch smell and taste (Bromley, Hare, Davison & Emerson, (2001). • Individuals show abnormalities across multiple domains (Rogers, Hepburn, Wehner 2003; Baranek, David, Poe, Stone & Watson 2006).
Sensory Environments • There is limited information which claims better concentration is observed after multisensory sessions (Lindsay, Pitcaithly, Geelen, Buntin, Broxholme & Ashby, 1997). • A recent single case study of three adults with a diagnosis of ASD reported fewer prompts required in a preferred activity for 2 out of the three participants (Kaplan, Clopton, Kaplan, Messbauer & McPherson, 2006).
Sensory environments • The effects of multi-sensory environments appears to indicate that increased relaxation and reduced overt signs anxiety can be achieved (Stephenson, 2002; Lancioni, Cuvo & O’Reilly, 2002). • Reduction in the frequency of aggressive behaviour of two individuals with ASD and no effect on a third person has been reported (Kaplan, Clopton, Kaplan, Messbauer & McPherson, 2006).
Definition of low arousal approaches • “A collection of behavior management strategies which focus on the avoidance of confrontation. This is primarily achieved by the reduction of triggers / cue behaviors which may arouse an individual who presents with challenging behaviours.’ McDonnell, Waters & Jones (2002)
Key Elements • Demand reduction in crisis situations. • Reduction in environmentally arousing stimuli. • Awareness of non verbal communication. • Diversionary tactics. • Challenging staff assumptions about the individuals control of their behaviour.
External (environmental) factors • Crowding. • Temperature. • Noise. • Use of stimulants (caffeine). • Staff/service users behaviour. • Level of exercise. • Visual design of environments
Internal factors • Damasio and Maurer, (1978) produced a neurological model for childhood autism. They argued that areas of the temporal area and mesolimbic systems were implicated in autism. • Studies have also attempted to identify structural areas of the brain implicated in sensory differences particularly the limbic system involving the hippocampus and the amygdala (Lathe, 2006).
Internal factors • There is laboratory research which demonstrates the relationship between an individuals levels of physiological arousal and performance in learning. • Studies of human performance have documented the relationship between behavioural performance and anxiety. • High levels of physiological arousal may impair cognitive processing in some individuals with ASD.
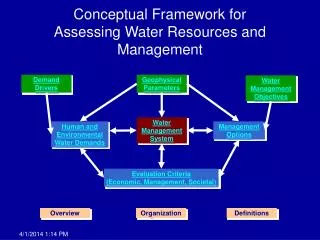
Maintaining Equilibrium: A central tenet. A balance between internal and external stimuli is required to maintain levels of arousal.
Equilibrium/balance • The human body has a sensitive self-monitoring and self-regulating system that is constantly working to maintain the body in homeostasis (balance). • I would suggest that physiological arousal employs a similar mechanism. A balance is struck between internal and external sources of arousal. Let us call it arousal homeostasis. • Each individual has an optimum performance threshold of arousal to functioning successfully. • We are aiming for a state of arousal equilibrium. • Regulation of arousal is problematic for some people with ASD.
Maintaining equilibrium • Stereotyped movements may help maintain equilibrium because they serve a de-arousing function. • Rituals may occur more frequently when arousal levels increase. • People avoid specific arousing stimuli. • Other do individuals seek out arousing stimuli.
Challenging behaviour and panic reactions • Many people with ASD and challenging behaviours show signs of panic in specific situations. • Behaviours may be interpreted as deliberate by carers in these situations • Similarities have been drawn between the symptoms of post traumatic stress disorder and some individuals who present with challenging behaviours (Pitonyak, 2004). • Panic reactions can often lead to people needing to escape from situations. • Panic responses do not appear to habituate rapidly. This may be true of a specific subset of people with ASD.
Physical Interventions • Some individuals may try to avoid physical contact. These individuals are often hypersensitive to tactile stimuli. • Any physical contact can have the potential to cause major distress in these circumstances. • Some persons may even experience light touch as physically painful (See Grandin & Scariano, 2002).
Physical Interventions • I have worked with individuals who seek out forms of restraint such as spine and prone holds . • Temple Grandin described the calming effect of deep pressure contact for her. • Some individuals may be of increased risk of harm especially if they show low initial reactivity to painful stimuli.
High arousal approaches? • Some individuals may show very low reactivity to environmental stimuli. • In these cases low arousal levels effect initiation and regulation of movement • ‘Catatonia’/ profound movement differences are relatively rare. • Clinically, some individuals appear to require increases in environmental arousal to help them ‘move’.
Measurement of arousal • Measuring physiological arousal can be difficult in people with ASD. • Cortisol levels (MacCreadie, 2007). • Variations in systolic and diastolic blood pressure. • Heart rate monitoring in the presence of specific arousing sensory stimuli. • Habituation responses to specific stimuli. • Functional assessment of sensory processing modalities. Where ethically appropriate some limited behavioural testing should be adopted.
Conclusions • Sensitivity to arousal as a model of working has several implications. • We are aiming to create ‘arousal equilibrium’ for individuals. • Assessment of individual arousal sensitivity should be a fundamental part of the approach. • Pharmacological approaches may need to concentrate more on reducing or in some cases increasing physiological arousal.
Conclusions • Designing environments where arousal levels can be controlled (heat, light, colour, space, sounds). • Developing more self control distraction strategies (wearing walkmans, use of mood music). • Anxiety reduction strategies may help some individuals (see Attwood, 2006). • Consider individual arousal responses when developing individualised activity plans.
Conclusions • The behaviour of staff has significant impact on the management of challenging behaviours. • Staff may inadvertently trigger challenging behaviours (McDonnell, 2005) • Training staff/families to recognise the initial signs of panic and sensitivity may have a significant effect. • Short term demand reduction should be a major facet of crisis management for people with ASD.
Presentation availability • For a copy of this presentation or further information please use the studio3 forum. • www.studio3.org.