Download
1 / 24
450 likes | 3.58k Views
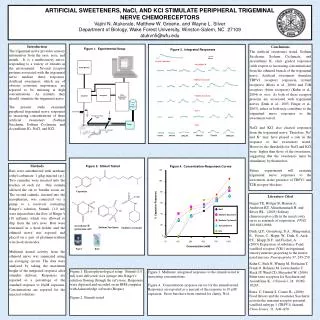
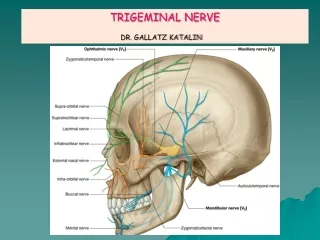
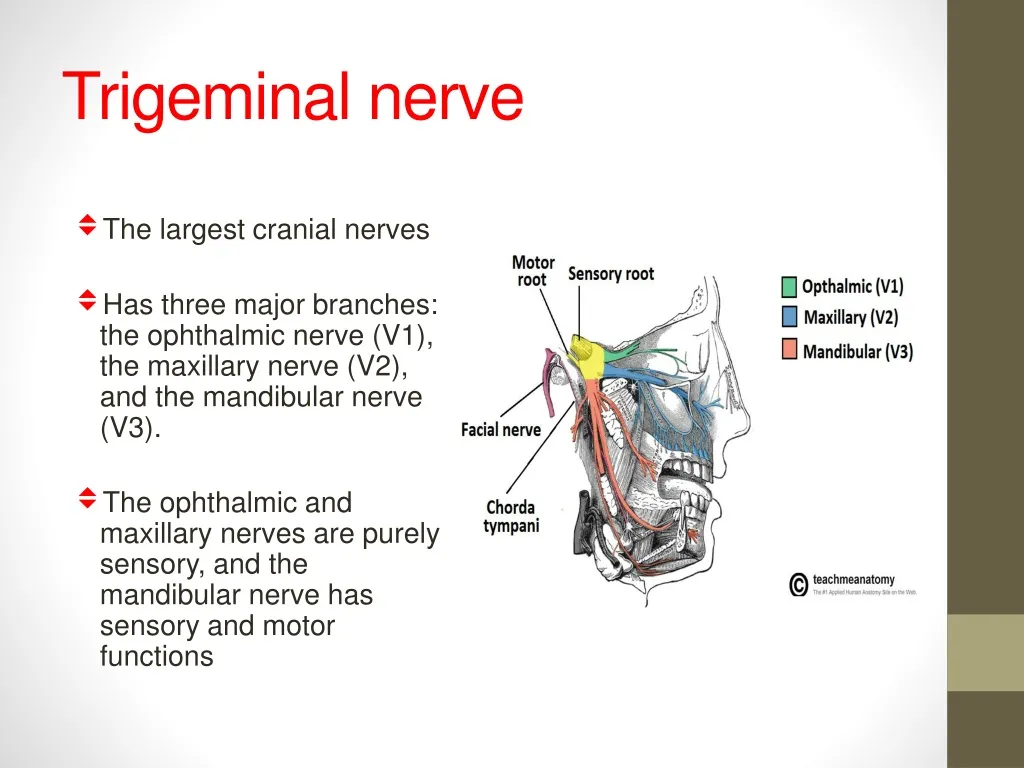
Trigeminal nerve. The largest cranial nerves H as three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). The ophthalmic and maxillary nerves are purely sensory, and the mandibular nerve has sensory and motor functions. Trigeminal nerve.

E N D
Trigeminal nerve • The largest cranial nerves • Has three major branches: the ophthalmic nerve (V1), the maxillary nerve (V2), and the mandibular nerve (V3). • The ophthalmic and maxillary nerves are purely sensory, and the mandibular nerve has sensory and motor functions
Trigeminal nerve • The three major branches of the trigeminal nerve converge on the trigeminal ganglion located within Meckel's cave • From the trigeminal ganglion a single, large sensory root enters the brainstem at the level of the pons. • The sensory function of the trigeminal nerve is to provide tactile, proprioceptive, and nociceptive afference to the face and mouth.
Trigeminal nerve • In the pons face represented as onion skin distribution differs from the dermatome distribution of the peripheral branches of the fifth nerve. • Lesions of pontine portion of trigeminal nucleus resulting in loss of sensation in the nose upper lip and mouth only
Trigeminal nerve • The motor root emerges from the pons at the same level. Motor cell bodies are located in the nucleus of the fifth nerve, deep within the pons. • Its motor function activates the muscles of mastication ( temporalis, masseter, pterygoids) , all have bilateral cortical representation.
Etiology Brainstem: Cerebello-pontine angle: associated with other ipsilateral cranial nerve (e.g. VI, VII, VIII, IX), brainstem, and cerebellar signs. Acoustic or glossopharyngeal neuroma • Trigeminal neuroma • Meningioma lesions are often associated with other CN deficits and long tract involvement: • Stroke (lateral medullary syndrome). • Multiple sclerosis • Tumor
Etiology Meckel’s cave: Base of the skull: Meningitis (infectious, inflammatory, carcinomatous). Cavernous sinus associated with ocular motor (III, IV, and VI cranial) nerve palsies, Horner’s syndrome, optic nerve or chiasm compression, and sometimes pain above and within the orbit. Aneurysm of carotid siphon or ophthalmic artery. • Carotid–cavernous fistula. • Cavernous sinus thrombosis. • Sarcoidosis. • Tolosa–Hunt syndrome affect all divisions of CN V and VI(Gradenigo’s syndrome) • Schwannoma. • Meningioma. • Nasopharyngeal cancer Orbit (V1): Sensory disturbance in the first division only, associated with ophthalmoplegia. • Inflammation. • Cellulitis. • Tumor.
TRIGEMINAL NEURALGIA Is a painful condition caused by processes affecting the trigeminal nerve resulting in demyelination of its fibers. It is characterized by severe, paroxysmal, sharp lancinating pain in the distribution of one or more divisions of the trigeminal nerve (typically affecting V2 V3). • Incidence: 2–8 per 100,000 per year. • Age: usually starts after the age of 50 years, most commonly in the sixth and seventh decades. • Gender: FM (1.5:1).
TRIGEMINAL NEURALGIA TN is divided by the International Headache Society into two types: • Classic: idiopathic or presumed to be caused by vascular compression of the trigeminal nerve, most commonly by an aberrant superior cerebellar or anterior inferior cerebellar artery. • Symptomatic: due to an underlying cause other than vascular compression. This includes: • MS due to a plaque of demyelination at the root entry zone in the pons. This accounts for 2–3% of all cases of TN and up to 8% in younger patients. • Tumor • Arteriovenous malformations • Aneurysm • Herpes zoster
TRIGEMINAL NEURALGIA Clinical features imaging • Pain occurs in the face or mouth pain is described as brief (lasting for seconds) and followed by long pain-free intervals, and as stabbing/ lightning or electric shock-like/penetrating jabs of pain or clusters of stabbing pains. • Trigger points are areas around the nose, lips, or mouth when touched, evoke a paroxysm of pain. • Trigger factors include talking, chewing, swallowing, shaving, brushing the teeth, • The pattern is episodic: pain may recur several times a day for weeks or months, and then may remit for months or years.
TRIGEMINAL NEURALGIA Treatment Herpes zoster Medical: • Carbamazepine • Phenytoin • Baclofen • Gabapentin • pregabalin. • Lamotrigine Decompression Denervation • Percutaneous stereotactic radiofrequency thermal rhizotomy • Percutaneous glycerol rhizotomy. • Balloon compression of the trigeminal ganglion. • Intracranial nerve section of the appropriate divisions
Facial nerve Anatomy(Intracranial) Arises in the pons, as two roots: • Large motor root • Small sensory root The two roots travel through the internal acoustic meatus they are in very close to the inner ear. The roots leave the internal acoustic meatus, and enter into the facial canal
Facial nerve Facial canal The two roots fuse to form the facial nerve & forms the geniculate ganglion It give rise to : • greater petrosal nerve (parasympathetic fibres to glands) • Nerve to stapedius • Chorda tympani (special sensory fibres to the anterior 2/3 tongue). The facial nerve then exits the facial canal (and the cranium) via the stylomastoid foramen.
Facial nerve Extracranial Function Motor: Innervates the muscles of facial expression, stylohyoidand the stapedius muscles. Special Sensory: Provides special taste sensation to the anterior 2/3 of the tongue. Parasympathetic: Supplies many of the glands of the head and neck, including the submandibular, sublingual, nasal, palatine, lacrimal and pharyngeal gland.
Clinical relevance Intracranial Lesions • The muscles of facial expression will be paralyzed or severely weakened. The other symptoms produced depend on the location of the lesion, and the branches that are affected: • Chorda tympani – reduced salivation and loss of taste on the ipsilateral 2/3 of the tongue. • Nerve to stapedius– ipsilateralhyperacusis (hypersensitive to sound). • Greater petrosal nerve – ipsilateral reduced lacrimal fluid production. Extracraniallesions • weakness of the muscles of facial expression.
CAUSES OF UNILATERAL VII CRANIAL NEUROPATHY Pontine Infections Ramsay Hunt syndrome(HZV) Herpes simplex virus Meningitis Inflammatory Sarcoid Neoplastic Carcinomatous • Infarct • Multiple sclerosis • Brainstem tumor • Encephalitis • Abscess • Hemorrhage Tumor • Acoustic neuroma • Meningioma • Cholesteatoma • Metastatic • Parotid tumor
Bell’s palsy Epidemiology Clinical features posterior auricular pain decreased tearing hyperacusis taste disturbances Acute onset of unilateral LMN facial paralysis (over a 48-h period). • 23 per 100,000. • The right side is affected 63% of the time. • 29% higher with diabetes • pregnant 3.3 times higher • Bell palsy is thought to be caused by edema and ischemia resulting in compression of the facial nerve in its course through the bony canal • Herpes simplex virus (HSV) is the most likely cause.
Facial nerve Features other than Bell’s palsy UMN Facial weakness • sudden onset of hearing loss and severe pain with the onset of facial paralysis (Ramsay Hunt syndrome). • Recurrent ipsilateral facial paralysis or progressive paralysis of the facial nerve lasting longer than 3 weeks (neoplasm). • paralysis involves only the lower portion of the face (central cause).
Investigations • Imaging is not necessary • MRI of patients with Bell palsy may show enhancement of the seventh nerve • Neoplasm
Investigations EMG • useful when performed 3-10 days after the onset of paralysis. • A difference of 90% in amplitude between the paralyzed and normal sides suggests poor prognosis.
Bell’s palsy Medical care Surgical Care Decompression facial nerve less than 90% of normal activity by EMG Goals • reduce neuronal damage • improve function Treatment must be considered for patients of paralysis within 1-7 days of onset • corticosteroids • acyclovir • eye care • 80-90% of patients recover within 6 weeks to 3 months • poor prognostic signs: • age greater than 60 years • complete paralysis • decreased taste • hyperacusis, • decreased tearing.
Bilateral facial paralysis • 23% Bell palsy • Guillain-Barré syndrome • meningitis (neoplastic or infectious) • Syphilis • Leprosy • Lyme disease • Herpes simplex virus, herpes zoster virus • Sarcoidosis • Amyloidosis