Download
1 / 22
220 likes | 548 Views
New Onset Headache: Diagnosis and Management Michelle Biros MS, MD Dept. Emergency Medicine Hennepin County Medical Center. The Case. Visit One- A 20 year old woman presents with a headache for three days. Emesis x1. No photophobia, fever, URI symptoms or visual changes.

E N D
New Onset Headache:Diagnosis and Management Michelle Biros MS, MD Dept. Emergency Medicine Hennepin County Medical Center
The Case Visit One- A 20 year old woman presents with a headache for three days. Emesis x1. No photophobia, fever, URI symptoms or visual changes. Headache is severe, intermittent and throbbing, scalp / occiput, with radiation to the neck. No relief with OTC medications. PMHx- unremarkable; no prior headaches.
The Case (Continued) Afebrile 114/68, HR 76, in NAD General exam – normal PERRLA, EOMI, Fundi-normal Neck- supple Neurologic exam – normal Relief with IM droperidol, 2.5 mg. Increased neck pain, thought to be a dystonic rxn, resolved with benadryl. Dx: Tension HA vs Migraine vs Vascular
International Headache Society • A first episode of severe headache cannot be classified as migraine • Nor as tension-type headache • First or worst headache requires evaluation
Headache • 1 of 10 top presenting complaints in the USA • 1 to 2% of visits to ED • 18 million outpatient visits • 78% of women and 64% of men had at least one headache in the last year • 36% of women and 19% men suffer from recurrent headaches
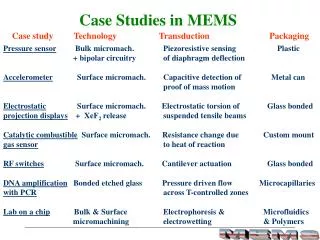
Types of Headaches in the ED Final Diagnosis Percentage • Infection - not intracranial 39.3 • Tension HA 19.3 • Miscellaneous 14.9 • Post-traumatic 9.3 • Hypertension related 4.8 • Vascular (Migraine) 4.5 • No diagnosis 6.0 • SAH 0.9 • Meningitis 0.6
The Case ( continued) One week later- Found unresponsive with shallow respirations. No response to Narcan. Blood sugar = 115. Husband states has had no recent fever, trauma or drug use. States she has had headaches all week, worst today on waking. She also c/o neck pain. Became lethargic over a few hours.
The Case ( continued) BP= 110/80: HR= 120: RR= 6: Afebrile GCS= 3+2+3= 8 General exam- Atraumatic: not protecting her airway Neuro- Pupils midposition, sluggish Corneals intact; sustained clonus Course: RSI, CT, OR
SAH: Most patients have... • Abrupt onset of severe, unique headache, or neck pain • Abnormal findings on neurologic examination • Subtle meningismus or ocular findings
SAH…But not “Classic” • Roughly half have minor bleeding with atypical features • Nonstrenuous activities (34%) • Sleep (12%) • HA in any location (localized, generalized, mild) • May be relieved by non-narcotic analgesics • Diagnosed as migraine, tension-type, sinusitis
Warning Headaches • 20 - 50% have HA days or weeks before index episode- sentinel bleed • “Thunderclap” headache Intense, acute, peak intensity at onset Develop in secs: Maximal intensity in mins Differential = SAH, Cerebral venous thrombosis, expansion of unruptured aneurysm, exertional HA
Intracranial Aneurysms • Women: men = 3 : 2 • 4 million Americans • 20% multiple aneurysms • Increase dx in mid-20s • Peak incidence of 12% by age 60 • Risk of spontaneous rupture 1 to 3%/yr • Peak 40 to 60 years
Arteriovenous Malformations • 10-15% of SAH • Spontaneous hemorrhage • Any age but usually < 30 • Incidence 3% per year • Incidence of major neurologic deficit or mortality: 50%
Physicians Consistently Misdiagnose SAH • Failure to appreciate spectrum of clinical presentation • Failure to understand limitations of CT • Failure to perform and correctly interpret the results of LP
Can a CT Scan Safely “Rule Out” SAH? • First diagnostic study • Thin cuts ( 3 mm) through base of brain • Blood on CT function of Hgb • Sensitivity decreases over time from onset of symptoms
Acute HA of Recent OnsetLeido A. Headache 1994 • 9 of 27 (33%) : SAH • 4 (+) CT • 5 normal CT, (+) LP • 2 of 19 LPs: meningitis • CT scanning and LP should be done with first severe acute headache
Morgenstern, et al: Ann Emerg Med 1998 • 455 headaches & 107 “worst headache” • CT: 18 of 107 (17%): (+) SAH • (-) CT/ (+) SAH by LP: Only 2 (2.5%) • Modern CT is sufficient to exclude 98% of SAH in patients
SAH: CT SensitivitySames: Acad Emerg Med Jan 1996 • 181 adult patients with SAH • Sensitivity 91.2% • Pain < 24 hrs 93.1% • Pain > 24 hrs 83.8% • LP 100% sensitive if CT (-) • “A normal NGCT does not reliably exclude the need for LP”
What about LP First? Duffy et al; 1982: 55 patients with LP first - 7 immediately deteriorated Hillman et al; 1986: 4 alert patients with SAH deteriorated after LP Both :Clots on CT dilated pupil Schull 1999; Math modeling- LP first at 12 hrs increases LPs by 9/100; reduces CTs by 81. Can use in selected patients.
Traumatic Taps • “Impression” or “3-tube” method not reliable to r/o trauma • Hgb bili, oxyhgb xanthrochromia • Best predictor of SAH in face of bloody tap ; timing important • Repeat tap , repeat CT, angiogram
Case • Assumed to have drug OD • Intubated, lavaged • SAH diagnosis entertained, CT • CT (+ ) blood everywhere • Angio OR
Lessons learned • First visit minimized • language barrier, mild sx, got better, neck pain administered • Second visit confusing • Paramedic assumptions carried over • History was most important