Download
1 / 40
1.07k likes | 4.69k Views
BRONCHOSCOPY. Cori Daines, MD Pediatric Pulmonology, Allergy and Immunology University of Arizona. BACKGROUND. Allows direct visualization of the airways Rigid and flexible instruments Clinical tool Airway anatomy Airway sampling Therapeutic Research tool. ORIGINS.

E N D
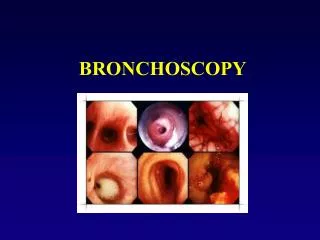
BRONCHOSCOPY Cori Daines, MD Pediatric Pulmonology, Allergy and Immunology University of Arizona
BACKGROUND • Allows direct visualization of the airways • Rigid and flexible instruments • Clinical tool • Airway anatomy • Airway sampling • Therapeutic • Research tool
ORIGINS • Until the 1980’s, only rigid instruments were widely used • Multiple generations of adult and pediatric flexible bronchoscopes now • Widely used in adult and pediatric pulmonary medicine now
RIGID BRONCHOSCOPY • Generally performed by ENT’s and surgeons • Procedure oriented • Foreign body removal • Biopsies • Granuloma/polyp removal • Laser • Stent placement • Visualization for future surgery
INSTRUMENTS • Rigid bronchoscopes • Hollow metal tube • Glass rod telescope • Ultimate optics
FLEXIBLE BRONCHOCSOPY • Examination of the entire respiratory anatomy, nose to bronchi • Minor impact on anatomy • Able to pass through an endotracheal tube or tracheostomy tube
INSTRUMENTS • Flexible instruments • Fiberoptic bronchoscopes • 2.2mm ultrathin • 2.8mm/1.2mm suction channel • 3.4mm/1.2mm suction channel • 4.4mm/2.0mm suction channel • 4.9mm/2.2mm suction channel • 5.9mm/3.0mm suction channel
INSTRUMENTS • Flexible instruments • Video bronchoscopes • 2.8mm/1.2mm suction channel (hybrid video scope) • 3.8mm/1.2mm suction channel • 4.0mm/2.0mm suction channel (hybrid video scope) • 4.9mm/2.0mm suction channel • 6.0mm/3.0mm suction channel • 6.3mm/3.2mm suction channel
Fiberoptic bronchoscope 2.8mm diameter
Pediatric Videoscope 2.8mm diameter
Pediatric videoscope 3.8mm diameter
Adult videoscope 4.9 mm diameter
INDICATIONS • When flexible bronchoscopy is the best, easiest, safest, most efficient way to obtain the information
TECHNIQUE • Anesthesia • Best accomplished in the operating room • May be performed bedside in an ICU setting • Continuous monitoring • Light anesthesia--allows continued spontaneous breathing • May be done with conscious sedation in older individuals
TECHNIQUE • Insertion • Nasal • LMA • Endotracheal tube • Tracheostomy tube • Appropriate topical anesthesia and lubrication
TECHNIQUE • Anatomical survey • Nasal passages • Pharynx • Larynx • Trachea • Bronchi • Examine all before any other procedures
TECHNIQUE • Additional procedures • Bronchoalveolar lavage • Brushings • Bronchial biopsy • Transbronchial biopsy • Laser • Others: cryotherapy, stent placement, foreign body removal, needle biopsy
BRONCHOALVEOLAR LAVAGE • Small aliquots of sterile normal saline instilled into the airway • Removed by suctioning • Samples distal bronchial and alveolar surfaces • Wedge position to prevent loss of fluid
BAL TESTS • Microbiology • Bacterial, viral, fungal, AFB, special techniques • Pathology • Cell count, differential, special stains
MICROBIOLOGIC STUDIES • Stains • Gram stain • Acid fast stain (Ziehl-Neelsen) • Antibody tests • Rapid tests, DFA tests • In-situ • PCR
SPECIAL STAINS • Lipid • Oil Red O • Sudan • Hemosiderin • Prussian Blue • Alveolar proteinosis • PAS • Electron microscopy
SPECIAL STAINS • Fungi • Silver (Gomori’s methenamine silver stain) • Pneumocystis carinii • Silver stain • Papanicolaou
SPECIFIC INDICATIONS • Atelectasis • Recurrent pneumonia • Chronic cough • Persistent/unexplained wheeze • Hemoptysis • Suspected airway compression/obstruction • Stridor • Upper airway obstruction • Suspected aspiration • Evaluation of tracheostomies
BRONCHOSCOPY TEAM • Pulmonologists • Respiratory therapists • Anesthesia • Nurses • Laboratory • Microbiology • Pathology