Download
1 / 39
420 likes | 724 Views
Fiberoptic Bronchoscopy in the ICU. R. Duncalf, MD, FCCP Pulmonary & Critical Care Division Bronx Lebanon Hospital Center. Introduction: Spectrum of Pulmonary Disease in the ICU. Pneumonia- community or nosocomial Pulmonary edema- cardiogenic or noncardiogenic

E N D
Fiberoptic Bronchoscopy in the ICU R. Duncalf, MD, FCCP Pulmonary & Critical Care Division Bronx Lebanon Hospital Center
Introduction: Spectrum of Pulmonary Disease in the ICU • Pneumonia- community or nosocomial • Pulmonary edema- cardiogenic or noncardiogenic • Pulmonary hemorrhage ± hemoptysis • Thromboembolic disease • Primary or metastatic CA • Interstitial lung disease • Obstructive airway disease • Respiratory failure in any of above requiring intubation and mechanical ventilation (MV) • Complications of intubation and MV
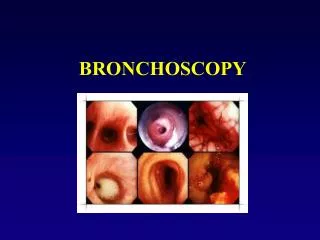
Introduction: Flexible Fiberoptic Bronchoscopy (FFB) • Essential diagnostic and therapeutic tool in ICU • Can be performed via endotracheal tube (ETT) or tracheostomy tube • Bedside procedure: avoids transport/ OR time
Common Diagnostic ICU Indications for FFB • Inspection, bronchoalveolar lavage (BAL), transbronchial lung biopsy (TBBx) • Abnormal chest X-ray/ suspected pulmonary infection • Hemoptysis • Lung carcinoma/ obstructing neoplasm • Chemical or thermal burns • ETT assessment/ management: intubation/extubation assist, position/ injury evaluation
Feng A, Sy E. A Lung Saddle Tumor. The Internet Journal of Pulmonary Medicine 2009 : Volume 11 Number 1 Elderly patient admitted with respiratory failure. Bx= Squamous cell Ca
Common Therapeutic ICU Indications for FFB • Retained secretions/ atelectasis • Mucous plugs- bronchial asthma, cystic fibrosis • Hemoptysis/ blood clots • Drainage lung abscess • Debridement of necrotic tracheobronchial mucosa • Dilation airway stenosis/ strictures
Indications in Critically Ill Medical Patients 198 bronchoscopies: 45% retained secretions 35% specimens for culture 7% airway evaluation 2% hemoptysis Olapade CS, Prakash U: Bronchoscopy in the critical care unit. Mayo Clin Proc 64:1255-1263, 1989
FFB in Pulmonary Infiltrates • Usually to evaluate infectious process • Allows directed sampling, identification of pathogens, de-escalation of antibiotics • BAL 10-50,000 CFU on culture diagnostic • protected specimen brush 5-10,000 CFU diagnostic • Potential for identification of noninfectious processes
Cos J, Sy E, Diaz-Fuentes G, Menon L. Foreign body presenting as a persistent lung infiltrate. The IJPM 2009 : Volume 11 Number 1
Cos J, Sy E, Diaz-Fuentes G, Menon L. Foreign body presenting as a persistent lung infiltrate. The IJPM 2009 : Volume 11 Number 1 After removal of foreign body
FFB in Retained Secretions and Atelectasis • FFB vs. physiotherapy for retained secretions: no superiority demonstrated • FFB in atelectasis: • retained secretions and air bronchograms to segmental level only • lobar or greater atelectasis not responding to aggressive chest PT • life threatening whole lung atelectasis • Severe hypoxemia not contraindication • Expect improved A-a gradient, static compliance, radiography (8 hrs)
3/24/10 3/26/10
Emergent FFB in the ICU • 27% atelectasis/ retained secretions • 17% ARDS/ pulmonary edema • 13% airway stenosis/ tracheobronchomalacia • 13% pneumonia/ empyema • 8% hemoptysis • 8% foreign body Hasegawa S, Terada Y, Murakawa M, et al: Emergency bronchoscopy. Journal of bronchology 5: 284-287, 1998
CXR after difficult intubation. Septic shock with MOD and AIDS
Daniel V, DeLaCruz A, Diaz-Fuentes G. Tracheal Laceration Due to Endobronchial Intubation. Journal of Respiratory diseases. June 2007:15-17
FFB: Complications • Premedication/ local anesthesia: respiratory depression/ arrest, methemoglobinemia, death • Procedure related: hypoxemia, cardiac complications, pneumonia, death • Ancillary procedures: barotrauma, pulmonary hemorrhage, death
Complications: Hypoxemia • Common: up to 2 hrs. post procedure: 20-30 mmHg O2 drop in healthy, 30-60 in critically ill • Reduction in effective tidal volume and FRC • Suction at 100mmHg via 2mm suction port removes 7L/min • Saline/lidocaine instillation
Safety of BAL in Ventilated Patients With ARDS J Bronchol Volume 14, Number 3, July 2007 148 ventilated patients with ARDS in ICU underwent FOB-BAL for investigation of VAP No deaths or major complications occurred in relation to BAL Only 2 minor episodes of desaturation (fall in SpO2 of 6%) occurred within two hours after BAL, a complication rate of 1.4% (P=0.49) FFB with BAL in ICU in ventilated ARDS patients (even with extreme hypoxemia ) is safe provided adequate precautions are taken
Complications: Cardiac • Hypoxemia, hypercapnea increased sympathetic tone arrhythmias, ischemia, hypotension death • Major arrhythmias in 11% • Unstable angina, severe preexisting hypoxemia risk factors • Hemodynamics: 30% MAP, 43%HR, 28% CI
FFB in MV: Physiology • Standard ED 5.7mm scope occludes 10% cross sectional area of trachea, 40% 9mm ID ETT, 51% 8mm ID ETT, 66% 7mm ID ETT • Hypoventilation, hypoxemia, gas trapping/ high intrinsic PEEP • 8mm ID ETT for standard scope recommended • Ultrathin bronchoscopes (2.8mm): reduce potential for hypoxemia/hypercapnea, dynamic hyperinflation
FFB in MV: Increased Complication Risk • Pulmonary: • PaO2< 70mmHg with FiO2> 0.7 • PEEP> 10 cm H2O • autoPEEP > 15 cm H2O • active bronchospasm • Cardiac: • recent MI (48 hrs.) • unstable arrhythmia • MAP < 65mm Hg or vasopressor • CNS: • increased intracranial pressure
FFB in MV: Complication Rates • < 10 % • Minor complications: 6.5% • Major complications: 0.08-0.15% • Mortality: 0.01-0.04% • Raoof S, Mehrishi S, Prakash U. Role of bronchoscopy in the modern medical intensive care unit. Clin Chest Med 2001; 22: 241-261
FFB in MV: Complications of TBBx • Study of 83 lung biopsies: • 14.3% pneumothorax • 8.4% hypoxemia < 90% • 7.2% hypotension (MAP < 60mm Hg) • 6% hemorrhage > 30 cc • 3.6% tachycardia >140/min. O’Brien JD, Ettinger NA, Shevlin D et al: Safety yield of transbronchial lung biopsy in mechanically ventilated patients. Crit Care Med 25: 440-446 1997
Yield and Safety of FFB and TBBX on patients on Mechanical Ventilation in the ICU Division of Pulmonary and Critical Care Medicine, Bronx- Lebanon Hospital Center, Bronx, NY
There is limited information on the usefulness and safety of TBBx in ICU patients on MV • The goals of the study were to evaluate the yield, safety and efficacy of FFB with BAL and TBBx compared to FFB-BAL only • Retrospective review of ICU patients on MV who underwent diagnostic FFB from January 2006 to December 2007 • TBBx was done at the bedside and without fluoroscopic guidance • The average number of biopsies per patient were 2 (range 1-3) • Patients who underwent FFB for inspection and / or therapeutic bronchoscopy were excluded
Demographics • 132 patients were identified: 92 in the BAL and 40 in the BAL with TBBx group • 48 (36%) of patients were HIV positive, all had AIDS • The main indications for FFB were evaluation of lung infiltrates (99%) and lung masses
Comparison of yield between HIV and Non HIV group P value= 0.04 P value= 0.9
Analysis of the yield for the BAL with TBBx positive in the Non-HIV patients
Analysis of yield for the BAL with TBBx positive in HIV patients
Results • There was no statistical difference in the yield from BAL when compared to BAL with TBBx for patients on MV • BAL alone showed a higher yield in patients with HIV as compared to non- HIV patients • More patients in the HIV positive group had BAL with TBBx compared with the non-HIV group ( 48% vs 20 % respectively) • TBBx revealed additional diagnosis in 4 patients: PCP (1), malignancy (1), and fungal infection (2) • There were no complications in either group
Conclusions • The overall yield of diagnostic BAL with TBBx was 60%; this lower than reported yield could be due to inadequate biopsy sampling due to the non-fluoroscopic technique and/or to the fewer number of biopsies done • TBBx is a useful alternative for the diagnosis of infections in critically ill patients who are too ill for surgical biopsies; especially in HIV+/AIDS patients where fungal infection is often a consideration • We recommend considering BAL with TBBx in selected patients on MV, especially in HIV+/ AIDS patients, where opportunistic infections are suspected • FFB with BAL with TBBx seems to be a safe diagnostic tool in ICU patients on MV