Download
1 / 36
360 likes | 687 Views
OBJECTIVES. To discuss the pathophysiologic impact of intrathoracic (ITP) and intra-abdominal (IAP) onPreloadContractilityAfterloadOxygen TransportTo consider the therapeutic interventions necessary to correct cardiac dysfunction. SETTING THE STAGE FOR IAH / ACS. Preload, contractility, afterload, and oxygen transport are commonly abnormal in the critically ill Subsequent development of sepsis, shock, or acute lung injury can further worsen cardiac functionInadequate resuscitation and fai224

E N D
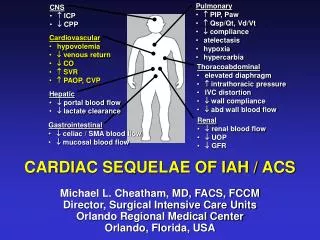
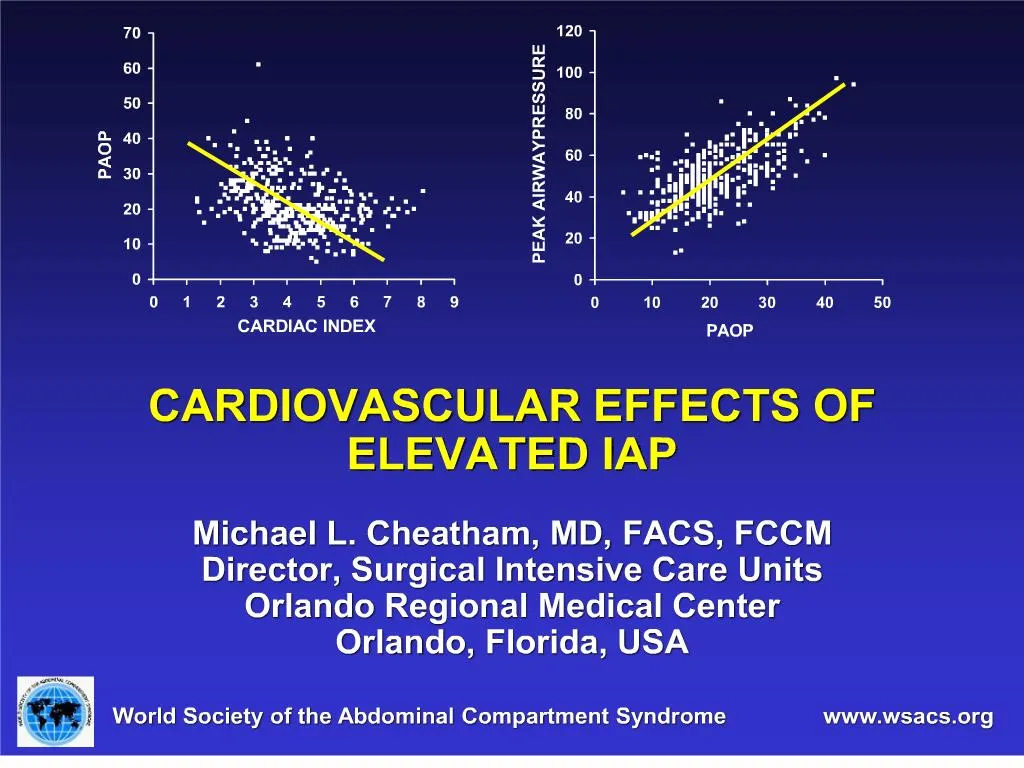
1. CARDIOVASCULAR EFFECTS OF ELEVATED IAP
Michael L. Cheatham, MD, FACS, FCCM
Director, Surgical Intensive Care Units
Orlando Regional Medical Center
Orlando, Florida, USA
2. OBJECTIVES To discuss the pathophysiologic impact of intrathoracic (ITP) and intra-abdominal (IAP) on
Preload
Contractility
Afterload
Oxygen Transport
To consider the therapeutic interventions necessary to correct cardiac dysfunction
3. SETTING THE STAGE FOR IAH / ACS Preload, contractility, afterload, and oxygen transport are commonly abnormal in the critically ill
Subsequent development of sepsis, shock, or acute lung injury can further worsen cardiac function
Inadequate resuscitation and failure to restore cellular oxygen delivery leads to
Ischemia
Anaerobic metabolism
Multiple organ dysfunction syndrome (MODS)
Death
4. SYSTEMIC EFFECTS OF IAH / ACS
5. THE IMPACT OF ITP AND IAP Elevated ITP and IAP cause
Cephalad deviation of the diaphragm
Cardiac compression
Pulmonary compression
Can have marked effects on preload, contractility, afterload, and oxygen transport
6. PRELOAD Adequate intravascular volume is essential
Loss of intravascular volume may be either
Absolute
Hemorrhage
Third-space fluid losses
Relative
Mechanical obstruction to blood flow
Anatomic
Pressure-induced
Thrombosis
7. PRELOAD Cephalad elevation of the diaphragm
Induces narrowing of the inferior vena cava (IVC)
Reduces blood return to the heart
Elevated IAP
Compresses the IVC
Limits blood return from below the diaphragm
Causes lower extremity and pelvic blood pooling
Promotes both genital and lower extremity edema
Places patient at risk for deep venous thrombosis
Such changes may occur with an IAP of 10 mmHg
8. PRELOAD Inadequate venous return decreases cardiac output (CO) through decreased stroke volume (SV)
CO reduction is proportional to volume status
Hypovolemic patients sustain CO reductions at lower levels of IAP than do normovolemic patients
Hypervolemic patients demonstrate increased venous return in the presence of elevated IAP
Volume resuscitation can to a point overcome both the anatomic and pressure-related restrictions to venous return restoring SV and CO
9. PRELOAD ASSESSMENT IN IAH/ACS Cardiac preload is commonly assessed using central venous pressure (CVP) or pulmonary artery occlusion pressure (PAOP)
Their use is based upon several assumptions:
Intermittent measurements reflect a patient�s continuously changing hemodynamic state
PAOP & CVP accurately reflect end-diastolic volume
Ventricular compliance is unchanging
10. THE PAOP ASSUMPTION
11. TRANSMURAL FILLING PRESSURES Resuscitation to arbitrary, absolute PAOP or CVP values should be avoided
Transmural pressures may be of greater accuracy
PAOPtm = PAOPee - Ppl
CVPtm = CVPee � Ppl
Substituting IAP for Ppl may provide a rapid bedside estimate of transmural filling pressure
12. IS THE PAC FLAWED OR ARE WE? Various studies have demonstrated that�
47% of physicians cannot derive basic hemodynamic information from a PAC
33% cannot identify a PAOP tracing
33% cannot describe how to increase a patient�s oxygen delivery
Is it any surprise that prospective trials have failed to demonstrate a survival benefit with the use of this device?
13. IS THE PAC REALLY FLAWED? Friese et al. Crit Care Med 2006; 34:1597-1601
Retrospective database analysis of 1,933/53,312 trauma patients managed with a PAC
PAC use led to significantly decreased severity-adjusted mortality in patients with:
ISS = 25 and base deficit > 11
Age > 61 years and base deficit > 6
PAC use improves survival in trauma patients with severe shock at the time of admission
Suggests that early goal-directed resuscitation using a PAC has a survival benefit that may have been missed by previous smaller trials
14. Mixed venous oximetry (SvO2) (1980�s)
Assessment of oxygen transport balance
Volumetric technology (1990�s)
Assessment of right heart function
Right ventricular ejection fraction (RVEF)
Right ventricular end-diastolic volume (RVEDVI)
A volumetric, as opposed to pressure-based, estimate of intravascular volume status
Superior to PAOP & CVP in predicting preload recruitable increases in CO
17. THE BENEFITS OF GOAL-DIRECTED RESUSCITATION USING A PAC
18. ARE WE MISSING TOO MUCH? Significant physiologic changes may go undetected by conventional intermittent monitoring techniques
A �snapshot� in time when a �moving picture� is what is needed
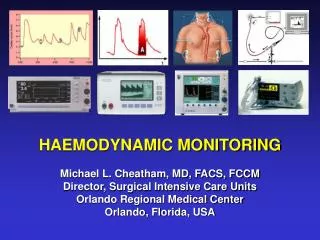
19. CONTINUOUS THERMODILUTION Utilizes pulsed thermal energy technology
Provides an updated hemodynamic assessment every 60 seconds
Reduces measurement variability
Automates CO measurement
Averages respiratory cycle variation
Standardizes injection technique
Provides a constantly updated assessment of patient response to resuscitation leading to more efficient, goal-directed resuscitation
20. CONTINUOUS THERMODILUTION Most invasive and labor-intensive of the monitoring technologies demanding a thorough understanding of PAC monitoring principles
Provides a continuous assessment of
Preload (RVEDVI)
Contractility (CO, RVEF)
Afterload (SVR, RVEF)
Oxygen transport balance (SvO2)
Improves patient resuscitation and outcome
Appropriate for the most critically ill patients
21. ARTERIAL PULSE CONTOUR ANALYSIS Estimation of SV from the arterial pressure waveform was first described almost 100 years ago
CO is proportional to the area under the arterial pressure waveform
Proposed as a less invasive alternative to the PAC
Requires only an arterial pressure catheter and a central venous catheter (CVC)
22. Accuracy is dependent upon arterial resistance, compliance, and impedance
Initial calibration via iced saline thermodilution
Recalibration every 8 hours
Provides continuous assessment of
Left ventricular SV and CO
Global ejection fraction (GEF)
Global end-diastolic volume (GEDV)
Intrathoracic blood volume (ITBV)
Extravascular lung water (EVLW)
Stroke volume variation (SVV)
ARTERIAL PULSE CONTOUR ANALYSIS
23. A less invasive alternative to a PAC
Provides continuous assessment of
Preload (GEDVI, ITBVI, EVLW, SVV)
Contractility (CO)
Afterload (SVR)
Multiple studies have demonstrated that CO correlates better with GEDVI and ITBVI than with PAOP in the presence of elevated ITP and IAP
A minimally invasive option for continuous hemodynamic monitoring in IAH/ACS ARTERIAL PULSE CONTOUR ANALYSIS
24. OPTIMAL RVEDVI / GEDVI Initial studies suggested an RVEDVI of 130-140 mL/m2 or GEDVI of 640-800 mL/m2 were optimal
This oversimplifies what is actually a complex and dynamic relationship
Ventricular function and compliance are constantly changing in the critically ill
RVEF / GEF must be considered when determining the optimal volume for resuscitation
End-diastolic volume ? 1 / Ejection Fraction
25. FAMILIES OF STARLING CURVES
26. CORRECTED TARGET VOLUMES
27. CONTRACTILITY Diaphragmatic elevation and direct cardiac / pulmonary compression�
Reduces biventricular preload
Elevates pulmonary artery pressures
Elevates pulmonary vascular resistance
In response, the thin-walled right ventricle dilates
The interventricular septum may bulge into the left ventricular chamber, impeding left ventricular function and decreasing cardiac output
May result in systemic hypotension and worsening right coronary artery blood flow
28. CONTRACTILITY At a time when right ventricular function is essential to maintaining CO
Right ventricular ejection fraction decreases
Right ventricular wall tension increases
Myocardial oxygen demand increases
Subendocardial ischemia may occur
Right ventricular dysfunction can become severe resulting in left ventricular failure due to "ventricular interdependence"
29. CONTRACTILITY Volume resuscitation and inotropic support will improve biventricular contractility at mild to moderate levels of IAH
Restores preload
Improves ventricular function
Increases coronary perfusion pressure
The cardiac dysfunction of severe IAH and ACS can only be reversed by decompressive laparotomy
Delayed intervention may prove to be futile
30. AFTERLOAD Generally increases to compensate for reduced venous return and falling SV
Elevated ITP and IAP pathologically�
Increases systemic vascular resistance through direct compressive effects on the aorta and systemic vasculature
Increases pulmonary vascular resistance through compression of the pulmonary parenchyma
31. AFTERLOAD Increased afterload is poorly tolerated by patients with�
Inadequate intravascular volume
Marginal cardiac contractility / prior dysfunction
Acute lung injury requiring PEEP
Preload augmentation appears to initially ameliorate the increased afterload
Decompressive laparotomy is most effective for reducing vascular resistance to appropriate levels
32. OXYGEN TRANSPORT Cellular delivery of oxygen is essential to avoiding multiple organ dysfunction
Efficient oxygen delivery requires appropriate
Preload
Contractility
Afterload
Alveolar oxygenation
Interventions aimed at reducing ITP and IAP are essential to improving oxygen delivery and transport balance
33. WSACS RECOMMENDATIONS Avoid overresuscitation
Fluid resuscitation volume should be carefully monitored to avoid over-resuscitation in patients at risk for IAH/ACS (Grade 1B)
Hypertonic crystalloid and colloid-based resuscitation should be considered in patients with IAH to decrease the progression to secondary ACS (Grade 1C)
Fluid resuscitation is a cornerstone of management
Consider goal-directed hemodynamic monitoring
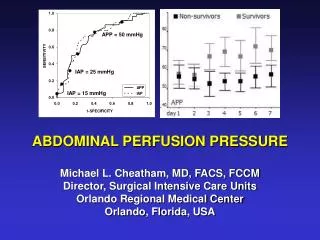
34. RESUSCITATION ALGORITHM Each patient should be resuscitated to restore end-organ function and normalize markers of perfusion adequacy
APP > 60 mmHg predicts survival from IAH / ACS
Unnecessary over-resuscitation should be avoided
May lead to secondary ACS, lung dysfunction
PAOP and CVP may be used to guide resuscitation with the explicit understanding that transmural estimates of PAOP and CVP must be utilized
35. CONCLUSIONS Cardiovascular dysfunction plays a major role in the organ dysfunction and failure that characterizes IAH/ACS
Optimal cardiac function is essential to avoiding multiple organ dysfunction and improving outcome
Preload, contractility, afterload, and oxygen transport balance are all interrelated
Correction of one component frequently mandates treatment of all
36. CONCLUSIONS Hemodynamic monitoring and goal-directed resuscitation are essential to improving patient outcome from IAH / ACS
PAOP and CVP are commonly erroneous in IAH
Reliance on such parameters may lead to under-resuscitation and inappropriate therapeutic interventions
Volumetric preload estimates such as RVEDVI and GEDVI are superior to PAOP and CVP as predictors of preload-recruitable increases in cardiac output