Download
1 / 14
140 likes | 258 Views
Pulmonary PIP, Paw Qsp/Qt, Vd/Vt compliance atelectasis hypoxia hypercarbia. CNS ICP CPP. Cardiovascular hypovolemia venous return CO SVR PAOP, CVP. Thoracoabdominal elevated diaphragm intrathoracic pressure IVC distortion wall compliance

E N D
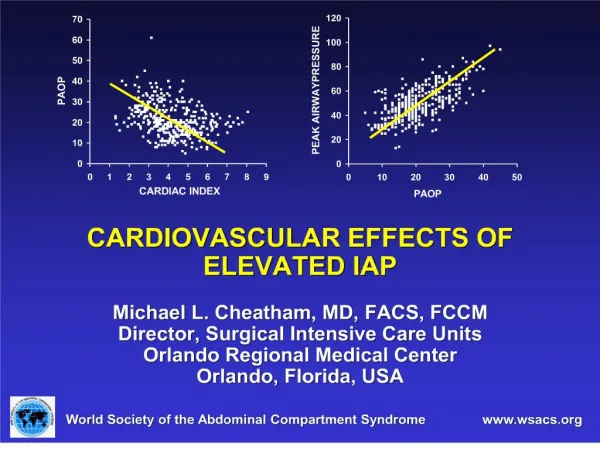
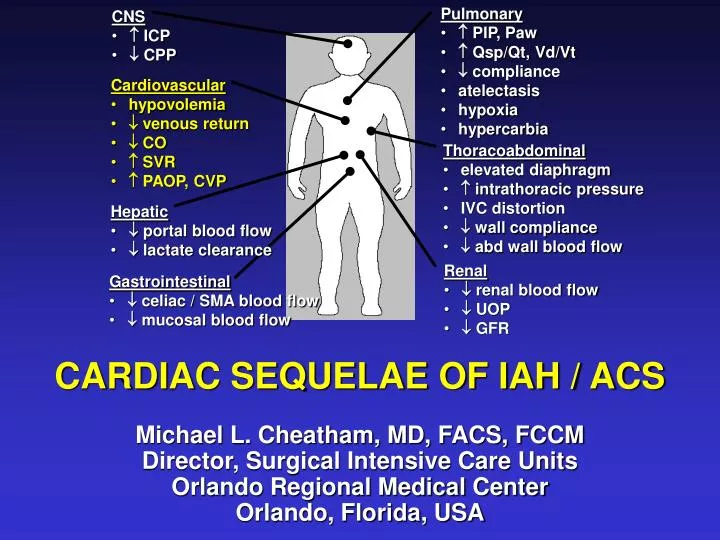
Pulmonary • PIP, Paw • Qsp/Qt, Vd/Vt • compliance • atelectasis • hypoxia • hypercarbia • CNS • ICP • CPP • Cardiovascular • hypovolemia • venous return • CO • SVR • PAOP, CVP • Thoracoabdominal • elevated diaphragm • intrathoracic pressure • IVC distortion • wall compliance • abd wall blood flow • Hepatic • portal blood flow • lactate clearance • Renal • renal blood flow • UOP • GFR • Gastrointestinal • celiac / SMA blood flow • mucosal blood flow CARDIAC SEQUELAE OF IAH / ACS Michael L. Cheatham, MD, FACS, FCCM Director, Surgical Intensive Care Units Orlando Regional Medical Center Orlando, Florida, USA
SETTING THE STAGE FOR IAH / ACS • Preload, contractility, afterload, and oxygen transport are commonly abnormal in the critically ill • Subsequent development of sepsis, shock, or acute lung injury can further worsen cardiac function • Inadequate resuscitation and failure to restore cellular oxygen delivery leads to • Ischemia • Anaerobic metabolism • Multiple organ dysfunction syndrome (MODS) • Death
THE IMPACT OF ITP AND IAP • Elevated intra-thoracic (ITP) and intra-abdominal pressure (IAP) causes • Cephalad deviation of the diaphragm • Cardiac compression • Pulmonary compression • Can have marked effects on preload, contractility, afterload, and oxygen transport
OBJECTIVES • To discuss the pathophysiologic impact of ITP and IAP on • Preload • Contractility • Afterload • Oxygen Transport • To consider the therapeutic interventions necessary to correct cardiac dysfunction
PRELOAD • Adequate intravascular volume is essential • Loss of intravascular volume may be either • Absolute • Hemorrhage • Third-space fluid losses • Relative • Mechanical obstruction to blood flow • Anatomic • Pressure-induced • Thrombosis
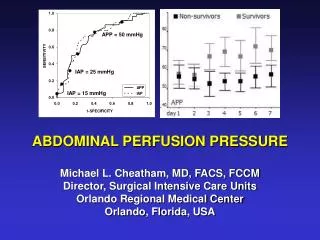
PRELOAD • Cephalad elevation of the diaphragm • Induces narrowing of the inferior vena cava (IVC) • Reduces blood return to the heart • Elevated IAP • Compresses the IVC • Limits blood return from below the diaphragm • Causes lower extremity and pelvic blood pooling • Promotes both genital and lower extremity edema • Places patient at risk for deep venous thrombosis • Such changes may occur with an IAP of 10 mmHg
PRELOAD • Inadequate venous return decreases cardiac output (CO) through decreased stroke volume (SV) • CO reduction is proportional to volume status • Hypovolemic patients sustain CO reductions at lower levels of IAP than do normovolemic patients • Hypervolemic patients demonstrate increased venous return in the presence of elevated IAP • Volume resuscitation can overcome both the anatomic and pressure-related restrictions to venous return restoring SV and CO
CONTRACTILITY • Diaphragmatic elevation and direct cardiac / pulmonary compression • Reduces biventricular preload • Elevates pulmonary artery pressures • Elevates pulmonary vascular resistance • In response, the thin-walled right ventricle dilates • Interventricular septum may bulge into the left ventricular chamber, impeding left ventricular function and decreasing cardiac output • May result in systemic hypotension, worsening right coronary artery blood flow
CONTRACTILITY • At a time when right ventricular function is essential to maintaining CO • Right ventricular ejection fraction decreases • Right ventricular wall tension increases • Myocardial oxygen demand increases • Subendocardial ischemia may occur • Right ventricular dysfunction can become severe resulting in left ventricular failure due to "ventricular interdependence"
CONTRACTILITY • Volume resuscitation and inotropic support will improve biventricular contractility at mild to moderate levels of IAH • Restores preload • Improves ventricular function • Increases coronary perfusion pressure • The cardiac dysfunction of severe IAH and ACS can only be reversed by decompressive laparotomy • Delayed intervention may prove to be futile
AFTERLOAD • Generally increases to compensate for reduced venous return and falling SV • Elevated ITP and IAP pathologically • Increases systemic vascular resistance through direct compressive effects on the aorta and systemic vasculature • Increases pulmonary vascular resistance through compression of the pulmonary parenchyma
AFTERLOAD • Poorly tolerated by patients with • Inadequate intravascular volume • Marginal cardiac contractility / prior dysfunction • Acute lung injury requiring PEEP • Preload augmentation appears to initially ameliorate the increased afterload • Decompressive laparotomy is most effective for reducing vascular resistance to appropriate levels
OXYGEN TRANSPORT • Cellular delivery of oxygen is essential to avoiding multiple organ dysfunction • Efficient oxygen delivery requires appropriate • Preload • Contractility • Afterload • Alveolar oxygenation • Interventions aimed at reducing ITP and IAP are essential to improving oxygen delivery and transport balance
CONCLUSIONS • Cardiovascular dysfunction plays a major role in the organ dysfunction and failure that characterizes IAH/ACS • Optimal cardiac function is essential to avoiding multiple organ dysfunction and improving outcome • Preload, contractility, afterload, and oxygen transport balance are all interrelated • Correction of one component frequently mandates treatment of all