Download
1 / 56
830 likes | 2.58k Views
IMAGING OF THE AXILLA. Dr. Varda Stahl-Kent Department of Radiology and the M. Fanny Breast Institute ASSAF HAROFE MEDICAL CENTER. WHY IS IMAGING OF THE AXILLA AN IMPORTANT PART OF BREAST IMAGING?. In cases of breast cancer axillary adenopathy has high correlation with prognosis.

E N D
IMAGING OF THE AXILLA Dr. Varda Stahl-Kent Department of Radiology and the M. Fanny Breast Institute ASSAF HAROFE MEDICAL CENTER
WHY IS IMAGING OF THE AXILLA AN IMPORTANT PART OF BREAST IMAGING? • In cases of breast cancer axillary adenopathy has high correlation with prognosis. • The number of nodes • The level of axillary involvement . • Extranodal extention
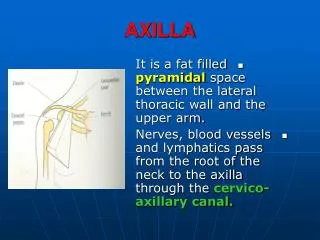
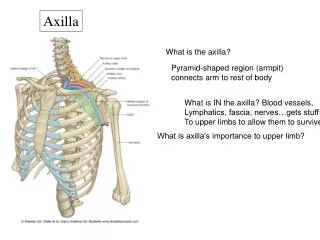
THE AXILLA -ANATOMIC BOUNDARIES • Anterior wall:pectoralis major and minor. • Posterior wall:subscapularis, latissimus dorsi and teres major muscles. • Medial wall: serratus anterior muscle. • Lateral wall: bicipital groove of humerus.
CONTENTS OF THE AXILLA • Fat, lymph nodes, arteries, veins and nerves. • Dense connective tissue that surrounds nerves and vessels. • May contain accessory breast tissue.
SURGICAL LYMPH NODE LEVELS • Level 1- low axillary group • L.N. lateral/inferior to pectoralis minor • Includes scapular, axillary vein and pectoral LOWER L.N. IN THIS GROUP ARE “SENTINEL” • Level 2 – Rotter nodes – mid-axillary group • Deep/posterior to pectoralis minor • Includes central and interpectoral and portions of subclavicular • LEVEL 1 AND 2 ARE INCLUDED IN ALND. • Level 3 – high or apical axillary group • Medial and superior to pectoralis minor
LYMPH NODES AND LYMPHATICS • 75% of drainage via lateral and medial trunks extending from areola to axilla • 25% via internal mammary chain • Anastomotic lymphatic channels may communicate with contralateral skin and breast.
IMAGING OF THE AXILLA • Should include axillary vein and artery, fat or breast tissue, lymph nodes and possible abnormality. • Accessory (ectopic) breast tissue in the axilla – common. • Benign and malignant primary tumors may occur in the axilla.
PHYSIOLOGY OF THE NORMAL LYMPH NODE • Blood enters and is drained through the hilum. • Afferent lymphatic channels enter through the capsule. • The fluid then flows to the subcapsular sinus, the cortical sinuses, and the l.n. mediastinum, to enter the medullary sinusoids. • When transcapsular arteries develop, it means that the l.n. bears metastases.
IMAGING AXILLARY L.N. WITH ULTRASOUND • Level 1, 2 and sometimes level 3 axillary nodes, and sometimes also internal mammary nodes can be seen. • Normal lymph node appearance • Usually elliptical, with long and short axes, hypoechoic cortex , hyperechoic fatty hilus. • May be longer than 2 cms. • Normal hilar vessels on Doppler exam. • Internal mammary nodes smaller than axillary, and morphology difficult to assess.
METASTASES TO AXILLARY L.N. • Malignant cells travel from breast to axilla in stepwise fashion. • Level 1 affected first, followed by 2 then 3. • Skip metastases <5%. • Likelihood of axillary involvement varies with location of breast primary. • Upper outer • Lower outer • Upper inner • Lower inner.
AXILLARY ADENOPATHY - IMAGING • Enlarged (usually >2 cm). • Absent or diminutive fatty hilum. • On mammography: Dense, rounded or irregular. • On ultrasound: Cortical thickening • Asymmetric - favors metastatic disease. • Uniformly thickened cortex - favors reactive adenopathy. • Spiculated margins suggest extranodal extension. • SHAPE IS MORE IMPORTANT THAN SIZE. • LONG TO SHORT AXIS RATIO <1.4 - PATHOLOGIC
AXILLARY ADENOPATHY – IMAGING (2) • Sensitivity for metastases 56 – 72%, specificity 70 – 90%. • Color Doppler: • Peripheral flow, transcapsular vessels favor malignancy (50% of nodes with peripheral flow – malignant, low likelihood of benign L.N)
ECCENTRIC CORTICAL THICKENING WITH OUTWARD AND INWARD BULGES
D.D. OF AXILLARY ADENOPATHY • Metastases from breast ca. • Other metastases – melanoma, lung, ovary, thyroid • Primary breast ca. • Silicone from current or prior rupture. • HIV • Lymphoproliferative diseases • Rheumatoid arthritis / collagen vascular diseases • Previous granulomatous infection – T. B., Histoplasmosis • Gold deposits • MALIGNANT ETIOLOGIES 55% • F.N.A. PERFORMED FOR EVALUATION
WORKUP OF AXILLARY ADENOPATHY • Clinical presentation of breast ca. as palpable axillary lymph nodes is rare (0.3 – 0.8%) • If F.N.A. positive for breast ca. and primary is not demonstrated, M.R.I should be performed • Even if primary is not demonstrated, the patient is treated as having an ipsilateral breast ca. • If F.N.A does not diagnose the cause for adenopathy, follow-up in 3 months.
DIAGNOSIS AND TREATMENT OF PATIENTS WITH AXILLARY METASTASES FROM BREAST CANCER • Sentinel lymph node biopsy performed intraoperatively if lymph nodes are not proven to contain metastases (by F.N.A or trucut biopsy) • If sentinel lymph node is affected- continue to ALND. • If more than 4 nodes affected – irradiation of the axilla
INTERNAL MAMMARY LYMPH NODES • Lie between the pleura and the intercostal muscles in the first to third intercostal spaces, within 1-2 cm of the lateral sternal border. • Adjacent to the internal mammary artery and veins. • Smaller than axillary L.N., about 0.6 cm. • About 20% of patients may have metastases to internal mammary lymph nodes, but usually axillary metastases occur first.
ACCESSORY BREAST TISSUE IN AXILLA • Ectopic breast tissue – mammary tissue that persists along the embriologic “milk line.” Accessory nipples and breasts may occur. • Physiologic changes may occur during menstrual cycle, pregnancy and postpartum. • Adenomas and fibroadenomas may occur. • Carcinoma may occur (less than 1% of breast carcinomas occur in the axilla)
CALCIFICATION WITHIN AXILLARY LYMPH NODES - D.D. • Granulomatous diseases – T.B, Histoplasmosis, sarcoidosis; fat necrosis. Usually coarse. • Metastatic breast ca. – amorphous and in peripheral location. • Extramammary metastases: ovarian, thyroid. • Gold deposits – can be punctate. • Silicone deposits.