Download
1 / 47
470 likes | 491 Views
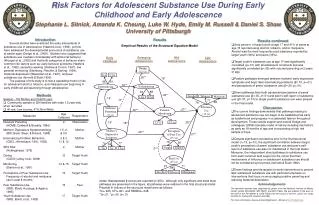
This article explores the historical perspectives, terminology, and different types of substances related to substance use and adolescence. It also covers the diagnoses, epidemiology, etiology, risk factors, course and prognosis, and treatment options for substance-related disorders.

E N D
Substance Use and Adolescence Edward S. Yuzda, MD, MSc, FRCPC (Psychiatry) Claude Ranger Mental Health Clinic Dec. 9th/04
Outline • Historical Perspectives • Terminology • Types of Substances • Diagnoses (DSM-IV) • Epidemiology • Etiology • Risk Factors • Course and Prognosis • Treatment
Historical Perspective • Since the first accidental discovery of beer and wine millennia ago, humankind has utilized substances for their psychoactive properties • The personality of the culture intertwined with and was influenced by the drug of choice for that era
Terminology • Drug vs.Substance • Legal vs. illegal • Addiction • Substance Dependence • Biological vs. Psychological Dependence
Types of Substances • Central Nervous Depressants • Alcohol • Cannabis • Sedative/hypnotics/anxiolytics • Opioid analgesics • Inhalants (ie. Glue/gasoline)
Types of Substances • Central Nervous Stimulants • Amphetamines • Caffeine • Cocaine • Nicotine • Ecstasy (mixed stimulant/hallucinogen)
Types of Substances • Hallucinogens • LSD • Mescaline • PCP
Types of Substances • Other • Gamma hydoxy butyrate (date rape drug) • Nitrite inhalants • Nitrous oxide • Kava • Betel nut • Nutmeg • Antihistamines • Antiparkinsonian drugs
Alcohol • By far the most common cause of substance related disorders in Canada • 50% of all fatal MVAs involve alcohol • 25% of all suicides involve alcohol • 1.5 oz. Spirits = 5 oz. Table wine = 12 oz. Beer = 3 oz. Fortified wine (13.6 grams of alcohol) • Intoxication can lead to blackouts/trauma/tolerance/ psychiatric symptoms
Amphetamine and Amphetamine-Like Drugs • Drastic increase in its use in 12-17 year olds over the past decade • Largely due to the popularity of the rave culture and designer rave drugs • Amphetamine related deaths have tripled in the 90’s • Serious psychiatric effects include psychotic symptoms
Caffeine • Most widely used psychoactive substance in the world • Present in pop/OTC medications/ chocolate/’pep’ pills • Meets criteria for abuse potential: • Positive reinforcer • Discriminated from placebo • Tolerance/withdrawal (yet not recognized by DSM-IV) • Largely associated with anxiety disorders
Cannabis • Most common illicit substance • Earliest recorded use (500BC) • Analgesic/anticonvulsant/hypnotic/anti-glaucoma/ appetite stimulant • 5% of people over age 12 have used cannabis within the past month • Use is on the rise after two decades of decrease • Good social drug • Controversy exists with regards to its psychiatric adverse effects (psychosis?/amotivation syndrome?)
Nicotine • An overlooked addiction • 1 billion users worldwide • Second to no other drug in its addictive potential • Use has steadily declined in the Western world secondary to extensive public education campaigns • Its use is a risk factor for use of other drugs
Diagnoses (DSM-IV) • Substance Use Disorders • Substance-Induced Disorders
Substance Use Disorders Substance Abuse Criteria A) A maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by any of the following criteria within a 12 month period: 1) symptoms lead to a failure to fulfill a major life role or obligation at work, home school 2) Repeatedly demonstrates intoxication when engaged in hazardous activities 3) Legal problems 4) cont’d use despite recurrent interpersonal/social consequence B) Never met criteria for substance dependence
Substance Use Disorders Substance Dependence Criteria A) Three or more of the following occurring at any time during a within a 12 month period: • Tolerance • Dependence • Takes larger quantities for longer times • Persistent unsuccessful efforts to cut down • Great deal of time spent trying to acquire the substance • All of daily activities are spent trying to obtain, use or recover from the effects of the substance • Cont’d use despite recurrent interpersonal/social problems Specify with/without physiological dependence
Epidemiology • 37% of people report to having used an illicit substance • 66% for people aged 16-25 • 15% of people over 28 have a serious substance use problem • 2/3 alcohol • 1/3 other drugs • 3.3% of 15 year olds meet criteria for substance abuse or dependence • The total cost of substance use problems is estimated at $200 billion/year
Epidemiology (cont’d) Male>Female Alcohol use : White=Hispanic>Black Marijuana use: Black>White
Epidemiology (cont’d) Use in past 12 months: Alcohol – 59.6% Nicotine – 27.6% Cannabis– 24.9% LSD – 7.6% Hallucinogens - 10.1% Stimulants – 6.6% Methamphetamine – 3.6% Ecstasy – 3.1% Cocaine – 2.7% Crack – 2.2% PCP – 2.0% Heroin – 1.8% Glue – 1.5%
Epidemiology (cont’d) Alcohol use (in past 12 months) 12th grade – 79.2% 10th grade – 71.8% 8th grade – 55.3% Alcohol ‘Drunk’ (in past 12 months) 12th grade – 61.8% 10th grade – 48.5% 8th grade – 26.8% Alcohol ‘regular use’ 12th grade – 30.2% 10th grade – 24.0% 8th grade – 15.6%
Epidemiology (cont’d) Cigarette use (in past 30 days) 12th grade – 34% 10th grade – 30% 8th grade – 21% Daily use 12th grade – 22.2%
Epidemiology (cont’d) Illicit drug use (in past 12 months) 12th grade – 40% 10th grade – 38% 8th grade – 24%
Epidemiology (cont’d) Marijuana use (in past 12 months) 12th grade – 36% 8th grade – 18% Daily Marijuana use 12th grade – 5%
Epidemiology (cont’d) LSD use (in past 12 months) 12th grade – 9% 8th grade – 4%
Epidemiology (cont’d) Amphetamine use (in past 12 months) 12th grade – 10% 8th grade – 9% Methamphetamine use (in past 12 months) 12th grade – 2.8% Ecstasy use (in past 12 months) 12th grade – 5%
Epidemiology (cont’d) Heroine use (in past 12 months) 12th grade – 1% 8th grade – 1.6%
Epidemiology (cont’d) Cocaine use (in past 12 months) 12th grade – 4.9% 8th grade – 3% Crack use (in past 12 months) 12th grade – 2.1% 8th grade – 1.8%
Number of people age 12 or older that have used illicit drugs in the past month (U.S.) Number of millions Year
Etiology • Psychological • Cultural • Genetic • Neurochemical
Individual-related Risk Factors • Early age of onset • Presence of early childhood behavioral problems • Poor academic performance • Risk-taking behaviors • Favorable beliefs about substance use • Shorter attention spans • Increased impulsivity • Increased irritability/emotionality
Family-related Risk Factors • Favorable beliefs about substance use in parents • Parental tolerance of substance use • Lack of closeness and attachment between adolescent and parent • Lack of discipline/supervision by parent • Parental substance use
Peer-related Risk Factors • Peer substance use • Favorable peer attitudes to use • Greater orientation of adolescents to peers as opposed to parents
Community-related Risk Factors • Low SE status • High population density • High crime rate
Natural History • Most adolescents try ‘gateway’ drugs (such as cigarettes or alcohol) which are legal and more accessible • such ‘gateway’ drugs then can lead to illicit drug use
Evaluation of a substance use problem • Evaluation includes: • Substance-use related behaviors • Observation of other psychiatric problems • School/vocational functioning • Family functioning • Social competency • Leisure activities • Medical status
Clinical indicators of a substance use problem • Psychosocial/behavioral • Change in school performance • Involvement in illegal activities • Sexual acting out (ie. Prostitution) • Increased demands for money • Change in peer group/involvement • Driving under the influence
Clinical indicators of a substance use problem (cont’d) • Medical • Frequent injuries • Suicide attempts • Sudden weight changes • Chronic respiratory symptoms • Gastrointestinal complaints • Insomnia • Infections • Anxiety • Depression • Sexually transmitted diseases
Clinical indicators of a substance use problem (cont’d) • Historical • Parental use • Estrangement from family • Poor quality relations in the family • Abuse/neglect • Psychiatric disorders • Early age of first use of substances
Clinical indicators of a substance use problem (cont’d) • Psychosocial behavioral • Change in school performance • Involvement in illegal activies • Sexual acting out (ie. Prostitution) • Increased demands for money • Change in peer group/involvement • Driving under the influence
Psychiatric Disorders Commonly Associated with Substance use disorders • Oppositional defiant disorder • Conduct disorder • ADHD • Mood disorders • Anxiety disorders • Bulimia nervosa • Schizophrenia • Personality disorders
Course and Prognosis • Most adolescents who use substances do not go on to develop problems • Levels of use often peak in late adolescence • Life events such as career attainment, education, marriage, parenthood tend to decrease substance use • Despite such maturational processes, substance use can disrupt the ability of adolescents to negotiate these tasks
Treatment • Young and socially stable patients have a better prognosis • Treatment can be divided into four phases: • Assessment and referral • Detoxification and withdrawal management • Active treatment • Continuing care
Treatment (cont’d) • Biological • Supportive medical measures • Treatment of withdrawal symptoms • Replacement pharmacological therapies (ie. Methadone) • Treat psychiatric co morbidities (ie. depression/ADHD/ etc.)
Treatment (cont’d) • Psychological • Twelve step programs (AA/NA) • Motivational interviewing • Cognitive behavioral therapy
Treatment (cont’d) • Social • Residential Programs : total control of adolescents environment • Intensive outpatient programs • Program characteristics associated with better outcomes include: • longer duration of Tx • available follow-up care • family involvement • social services
Treatment (cont’d) Prevention Direct vs. General (ie. Public health education campaigns) Successful prevention programs: target salient risk factors skills-oriented follow-up available culturally-oriented towards the targeted community