Download
1 / 1
10 likes | 163 Views
Ri sk Factors for Adolescent Substance Use During Early Childhood and Early Adolescence Stephanie L. Sitnick, Amanda K. Cheung, Luke W. Hyde, Emily M. Russell & Daniel S. Shaw University of Pittsburgh. Introduction

E N D
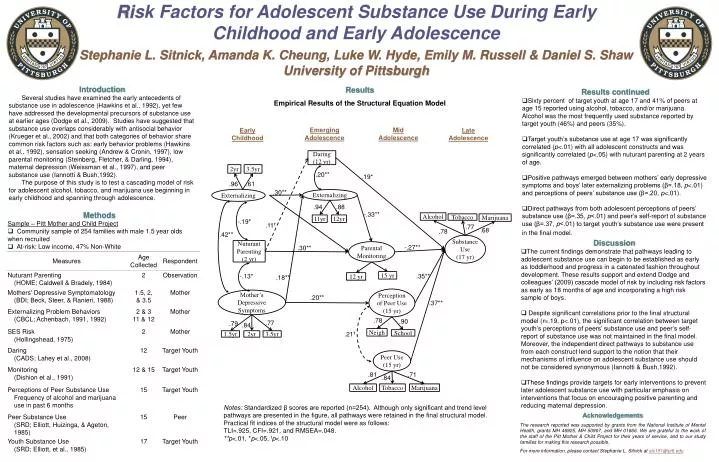
Risk Factors for Adolescent Substance Use During Early Childhood and Early Adolescence Stephanie L. Sitnick, Amanda K. Cheung, Luke W. Hyde, Emily M. Russell & Daniel S. Shaw University of Pittsburgh Introduction Several studies have examined the early antecedents of substance use in adolescence (Hawkins et al., 1992), yet few have addressed the developmental precursors of substance use at earlier ages (Dodge et al., 2009). Studies have suggested that substance use overlaps considerably with antisocial behavior (Krueger et al., 2002) and that both categories of behavior share common risk factors such as: early behavior problems (Hawkins et al., 1992), sensation seeking (Andrew & Cronin, 1997), low parental monitoring (Steinberg, Fletcher, & Darling, 1994), maternal depression (Weissman et al., 1997), and peer substance use (Iannotti & Bush,1992). The purpose of this study is to test a cascading model of risk for adolescent alcohol, tobacco, and marijuana use beginning in early childhood and spanning through adolescence. Results Empirical Results of the Structural Equation Model • Results continued • Sixty percent of target youth at age 17 and 41% of peers at age 15 reported using alcohol, tobacco, and/or marijuana. Alcohol was the most frequently used substance reported by target youth (46%) and peers (35%). • Target youth’s substance use at age 17 was significantly correlated (p<.01) with all adolescent constructs and was significantly correlated (p<.05) with nuturant parenting at 2 years of age. • Positive pathways emerged between mothers’ early depressive symptoms and boys’ later externalizing problems (β=.18, p<.01) and perceptions of peers’ substance use (β=.20, p<.01). • Direct pathways from both adolescent perceptions of peers’ substance use (β=.35, p<.01) and peer’s self-report of substance use (β=.37, p<.01) to target youth’s substance use were present in the final model. Emerging Adolescence Mid Adolescence Early Childhood Late Adolescence Daring (12 yr) 2yr 3.5yr .20** .19* .96 .61 .30** Externalizing Externalizing .94 .88 Methods -.33** Alcohol Tobacco Marijuana 11yr 12yr -.19* • Sample – Pitt Mother and Child Project • Community sample of 254 families with male 1.5 year olds when recruited • At-risk: Low income, 47% Non-White .11t .77 .68 .78 .42** Substance Use (17 yr) • Discussion • The current findings demonstrate that pathways leading to adolescent substance use can begin to be established as early as toddlerhood and progress in a catenated fashion throughout development. These results support and extend Dodge and colleagues’ (2009) cascade model of risk by including risk factors as early as 18 months of age and incorporating a high risk sample of boys. • Despite significant correlations prior to the final structural model (r=.19, p<.01), the significant correlation between target youth’s perceptions of peers’ substance use and peer’s self-report of substance use was not maintained in the final model. Moreover, the independent direct pathways to substance use from each construct lend support to the notion that their mechanisms of influence on adolescent substance use should not be considered synonymous (Iannotti & Bush,1992). • These findings provide targets for early interventions to prevent later adolescent substance use with particular emphasis on interventions that focus on encouraging positive parenting and reducing maternal depression. Nuturant Parenting (2 yr) Parental Monitoring -.27** .30** -.13* 15 yr .35** 12 yr .18** Perception of Peer Use (15 yr) Mother’s Depressive Symptoms .20** .37** .78 .90 .77 .79 .84 Neigh .21t School 1.5yr 2yr 3.5yr Peer Use (15 yr) .81 .71 .84 Alcohol Tobacco Marijuana Notes: Standardized β scores are reported (n=254). Although only significant and trend level pathways are presented in the figure, all pathways were retained in the final structural model. Practical fit indices of the structural model were as follows: TLI=.925, CFI=.921, and RMSEA=.048. **p<.01, *p<.05, tp<.10 Acknowledgements The research reported was supported by grants from the National Institute of Mental Health, grants MH 46925, MH 50907, and MH 01666. We are grateful to the work of the staff of the Pitt Mother & Child Project for their years of service, and to our study families for making this research possible. For more information, please contact Stephanie L. Sitnick atsls151@pitt.edu