Download
1 / 25
250 likes | 426 Views
Valuing prizes and making reimbursement decisions: how different?. Kalipso Chalkidou, MD, PhD Harkness Fellow in Health Policy Johns Hopkins School of Public Health on sabbatical from NICE (UK)

E N D
Valuing prizes and making reimbursement decisions: how different? Kalipso Chalkidou, MD, PhD Harkness Fellow in Health Policy Johns Hopkins School of Public Health on sabbatical from NICE (UK) DISCLAIMER: The views expressed here are those of the speaker and not of the Commonwealth Fund nor NICE.
What does NICE do? • Part of the National Health Service - UK • Issues evidence-based advice on clinical practice and the use of technologies • To make a decision it takes account of: • Clinical effectiveness • Cost-effectiveness: health/cost • Equity and other social values • Anti-discrimination and other legislation • Core principles: independence, transparency, inclusiveness, consistency, methodological robustness, review and appeal
Challenge 1 • Getting good quality unbiased evidence • Working with public sponsors of research • Working with industry early on in development • “Only in research’ and risk sharing -e.g. Velcade but… • Limited public funding for NICE priorities • Strong vested interests of sponsors • “Crowding out” of non-drug interventions when price discrimination by subgroup and indication is allowed
Challenge 2 • Applying the right threshold range • Annual health budget set by government normative decision • How much is an extra year in full health -one QALY- worth? positive decision given: • Health budget • Demand on budget by medical technologies • Empirical evidence of NHS productivity1 and of substitution of technologies at the local NHS level2 1: Martin S, The Health Foundation, 2007, 2: King’s Fund, Brunel and City Universities and NICE; also see Culyer A, J Health Serv Res2007
Challenge 3 • Incorporating values in decision-making • Equity and legal (UK, EU) considerations • Social Value Judgements and the Citizens’ Council • Case law -casuistry- approach within a framework of procedural justice: Daniels “accountability for reasonableness” • Always within the cost effectiveness range
Challenge 4 • What about the ‘innovation premium’? • Innovation matters: this is why we (NHS) pay up to £30,000 per additional QALY but we will not: • Settle for low quality or no evidence • Pay twice: once now and once when (if) the (better) innovation is developed • Give wrong incentives today leading to bad value innovation in the future • Compromise access today in hope of better (and possibly unaffordable) future medicines • Implicitly subsidise the drugs’ industry
UK developments in drug pricing “We recommend that Government reform the PPRS replacing current profit and price controls with a value based approach to pricing to ensure the price of drugs reflect their clinical and therapeutic value to patients and the broader NHS.” Office for Fair Trading, February 2007
UK government response “We agree with the OFT that it is time to develop a pricing system which is fit for purpose for the twenty first century. We must ensure that any future pricing scheme delivers value, rewards innovation and ensures a fair deal.” Interim Government Response to OFT Report Competitiveness Minister Stephen Timms, London, August 2007
The innovation debate • NICE and static efficiency: • as long as threshold reflects ‘real world’ productivity, and, • appropriate substitution takes place at local level • NICE and dynamic efficiency: • Signalling NHS demand curve to monopolist • Providing consistent evidence-based incentives which reduces undiversifiable, systematic risk (cost of capital) • Incentivising affordable future innovation
NICE methods and prizes: the same criticisms (i) • Who defines value? • The payer: payer’s WTP < patient’s WTA • How is value defined? • Incremental cost over incremental benefit + distributional and legal considerations • Hold-up (time inconsistency) problem • Transparent, consistent and reliable environment • Possibility of political rent seeking distorting research • Reality of private sector rent-seeking • Appropriate controls: public involvement and accountability • Publicly vs privately funded research: population need and capacity to benefit vs profit maximisation • Patent system notoriously bad in sharing information -commercial in confidence data DiMasi and Grabowski, 2004 and 2007
NICE methods and prizes: the same criticisms (ii) • Yardstick competition • Today: obscure costs and monopoly power • Benchmarking based on relative performance of similar firms (prizes) and of best alternative treatment (VBP) • Little experience • NICE, PBAC, PHARMAC…in operation for years • What about me-too (similar) drugs? • What about them?! DiMasi and Grabowski, 2004 and 2007
It’s not going to be easy…
A prizes’ approach would… • Disentangle the decision to develop an idea from the decision to purchase a product • Address access and rationing problems • only ‘worthwhile’ drugs enter the market • marginal cost pricing minimises deadweight loss • Incentivise investment in evidence-making, not marketing, to demonstrate value • Provide more secure investing environment (similar to P-V agreements in VBP)
Concluding remarks • Drugs’ markets already: • Centralised • Tax-funded in most countries: NICE (UK), PBAC (Aus), Cancer Care Ontario (Ca), HIRA (Kr)… • Prize setting and value-based reimbursement decision-making: • similar methodological principles (and criticisms) • we are becoming better in improving our methods and addressing the criticisms!
Selected publications • Martin, S, Rice, N and Smith, PC The link between healthcare spending and health outcomes: Evidence from English programme budgeting data, The Health Foundation, June 2007 • Culyer et al. Searching for a threshold, not setting one: the role of the National Institute for Health and Clinical Excellence. J Health Serv Res Policy. 2007 Jan;12(1):56-8. • S. Birch and A. Gafni. The 'NICE' approach to technology assessment: an economics perspective. Health Care Management Science 7 (1):35-41, 2004. • OTA, Pharmaceutical R&D: Costs, risks and rewards, Feb 1993 • Garber et al, Insurance and incentives for medical innovation, NBER, 2006 (paper 12080) • Claxton, K: OFT, VBP: QED?, Health Econ, 2007, 16: 545-558; (and forthcoming in the BMJ) • Gagnon, MA, Lexchin, J: The cost of purchasing pills, PLoS Medicine, Jan 2008, 5(1) • Light, D, Misleading Congress about drug development, 2007, Journal of Health Politics Policy and Law, 32(5):895-915, • DiMasi and Grabowski, Should the patent system for new medicines be abolished? Clin Pharmac Ther, 82(5): 488-490, Nov 2007; also: Comments on the Hubbard and Love trade Framewirrk for financing pharmaceutical R&D, June 2004 • M. D. Rawlins and A. J. Culyer. National Institute for Clinical Excellence and its value judgments. BMJ 329:224-227, 2004. • Skinner et al., Is Technological Change In Medicine Always Worth It? The Case Of Acute Myocardial Infarction, Health Affairs 25 2006: w34-w47 • A. Williams. What could be Nicer than NICE? London:Office of Health Economics, 2004. • Daniels N, Sabin JE: Limits to Health Care: Fair Procedures, Democratic Deliberation and the Legitimacy Problem for Insurers. Philosophy and Public Affairs 1997, 26(4):303-502.
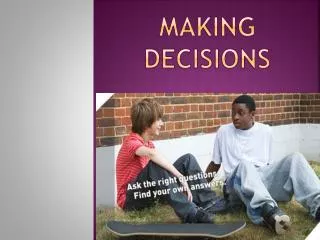
What are we giving up to pay for better value drugs? Webb and Walker, Lancet 2007
Bias? Lower ICER=Better value for money Miners et al, BMJ 2005
A4R • Publicity • Limit-setting decisions and their rationales must be publicly accessible. • Relevance • These rationales must rest on information and principled arguments that fair-minded parties (people predisposed to working together under rules of mutual cooperation) can agree are relevant to deciding how to meet the diverse needs of a covered population under necessary resource constraints. • Appeals • There is a mechanism for challenge and dispute resolution regarding limit-setting decisions, including the opportunity for revising decisions in light of further evidence or arguments. • Enforcement • There is either voluntary or public regulation of the process to ensure that the first three conditions are met. Daniels and Sabin, Philosophy and Public Affairs 1997
Some NICE Social Values • NICE should not recommend an intervention (that is, a treatment, procedure, action or programme) if there is no evidence, or not enough evidence, on which to make a clear decision. But NICE may recommend the use of the intervention within a data collection or research programme if this will provide more information about the effectiveness, safety or cost of the intervention. • Decisions about whether to recommend interventions should not be based on evidence of their relative costs and benefits alone. NICE must consider other factors when developing its guidance, including the need to distribute health resources in the fairest way within society as a whole. • Although NICE upholds the right of individuals to make their own decisions about their care, this should not lead NICE to recommend interventions that are not effective and cost effective enough to provide the best value to users of the NHS as a whole. • NICE recognises that when it is making its decisions it should consider the needs of present and future patients of the NHS who are anonymous and who do not have people to argue their case. • When choosing guidance topics, when developing guidance and when supporting people who are putting the guidance into practice, NICE should actively target health inequalities, such as those associated with sex, age, race, disability and socioeconomic status.
The innovation debate • Expected not current profits drive investment • Pharma no riskier than other R&D-driven industries • revenue (or profit) does not always mean R&D • R&D does not always mean health • Drug prices notonly tool for society to support R&D: tax regime, IPR regulations, infrastructure and education, direct funding (e.g NIH in USA) • Drug price notmost appropriate tool to support R&D: perverse effects on health, future innovation and industry through implicit subsidies to pharma OTA, 1993; Garber, NBER, 2006; Skinner, Health Affairs, 2006; Light, Public Health, Policy and Law, 2007 Claxton, Health Economics, 2007
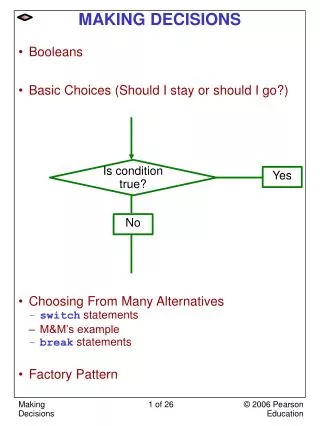
P P competitive firm Monopoly under patent protection demand demand Q In a market system, we get access to what we can afford… The market demand curve provides a constraint on a monopoly’s ability to profit from its market power. A monopolist would prefer, if it were possible, to charge a high price (P) and sell a large quantity (Q) at that high price. The market demand curve makes that outcome impossible. The monopolist can choose any point on the demand curve but it cannot choose a point off the demand curve. US: patients’ WTP, (obscure) insurance company and government criteria UK: NICE, local NHS-run Trusts Mankiw NG. Principles of Microeconomics, 4th Edition 2007
The momentum is building • France • EUnetHTA - EU Commission: evidence generation for new drugs • Drug pricing based on HAS tiers: economic evaluation considered • Germany • New Social Insurance Code: ceiling price on innovations • Economic evaluation by law - IQWiG (2007) • Korea • Positive list and value based pricing by law - HIRA (2008) • Italy • 5% tax on marketing to fund comparative effectiveness research • Used funding to compare b-IFN to azathioprine; latter better value • The Netherlands • Evaluation of all expensive inpatient and “orphan” drugs • Canada • PATH and THETA ‘field evaluations” of new technologies • Cancer Care Ontario