Download
1 / 34
340 likes | 620 Views
OutlineReview of the Structure and FunctionNasal Cavity, Pharynx, Trachea, Bronchi, Alveoli, LungsAge-Related ChangesTrachea and Bronchi, Alveoli, Lungs Structural ChangesAge-Related DysfunctionsChronic Obstructive Pulmonary DiseaseEmphysemaChronic BronchitisPneumoniaTuberculosisPulmonary Embolism.

E N D
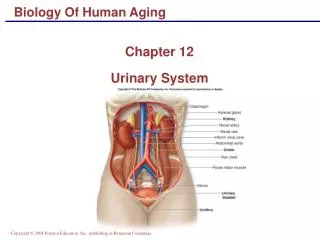
1. BIOLOGY OF HUMAN AGING Chapter 11
The Respiratory System
3. Human Respiratory System
Functions:
Works closely with circulatory system, exchanging gases between air and blood:
Takes up oxygen from air and supplies it to blood (for cellular respiration).
Removal and disposal of carbon dioxide from blood (waste product from cellular respiration).
Homeostatic Role:
Regulates blood oxygen and carbon dioxide levels.
4. Human Respiratory System
Components:
Nasal cavity, throat (pharynx), larynx (voice box), trachea, bronchi, alveoli, and lungs.
Pathway of Inhaled Air:
Nasal cavity
Pharynx (Throat)
Larynx (Voice Box)
Trachea (Windpipe)
Bronchi
Bronchioles
Alveoli (Site of gas exchange)
Exhaled air follows reverse pathway.
6. Pressure Relationships
8. Human Respiratory System
Nasal cavity: Air enters nostrils, is filtered by hairs, warmed, humidified, and sampled for odors as it flows through a maze of spaces.
2. Pharynx (Throat): Intersection where pathway for air and food cross. Most of the time, the pathway for air is open, except when we swallow.
3. Larynx (Voice Box): Reinforced with cartilage. Contains vocal cords, which allow us to make sounds by voluntarily tensing muscles.
More prominent in males (Adam�s apple).
9. Human Respiratory System
4. Trachea (Windpipe): Rings of cartilage maintain shape of trachea, to prevent it from closing. Forks into two bronchi.
5. Bronchi (sing. Bronchus): Each bronchus leads into a lung and branches into smaller and smaller bronchioles, resembling an inverted tree.
6. Bronchioles: Fine tubes that allow passage of air. Muscle layer constricts bronchioles. Epithelium of bronchioles is covered with cilia and mucus.
Mucus traps dust and other particles.
10. Human Respiratory System
Alveoli (Sing. Alveolus): Grapelike clusters of tiny air sacs with very thin elastic walls through which gas exchange occurs.
Oxygen in air enters blood in capillaries.
Carbon dioxide in blood enters air in alveoli.
There are several million alveoli in the human lungs, with a total surface roughly equivalent to a tennis court.
The walls of the alveoli are very delicate.
Alveolar macrophages are phagocytic cells that swallow inhaled particles (dust, bacteria, etc.) and digest them.
13. Lung volume and using spirometer
14. Lung volume and using spirometer
15. Age-related changes Trachea and Bronchi
Progressive calcification
Smooth-muscle replaced by fibrous connective tissue
Reduced elasticity of the lungs
VC begin to decrease ~ 40 years of age
Mucous membrane lining the trachea and bronchi show degenerative changes
Decrease activity of cilia and phagocytic activity of the macrophages
16. Age-related changes Alveoli
Gradual deterioration of the walls of alveoli
The size increases but less surface area for the gas exchange
Cross-linkage
More collagen fibers and less elastic fibers
Declining oxygen levels in the blood
17. Age-related changes Lungs
Lose their elastic recoiling capabilities and offer less resistance to expansion
Insufficient ventilation? contributing to an overall reduction in oxygen saturation of arterial blood.
Surface area
Diminished sensitivity of chemo-receptors that monitor oxygen and CO2 levels in the blood.
19. Age-related changes Structural changes
Kyphosis and the hunching over reduces the volume of the thoracic cavity and make it more difficult to expand the lungs
Loss of Ca and weakening of muscles
Diminished elasticity and increases fibrosis of the lungs
Stiffness of the rib cage
Older individual rely more on the diaphragm
20. Age-related dysfunctions
Dysfunctions of respiratory system are more common in older individuals
These are not merely a result of aging, rather due to constant exposure to environmental stimuli (air pollution & smoking)
Air pollutants damage trachea, bronchi, alveoli
Most frequently occurring pulmonary disorders:
Restrictive (hinder lung expansion)
Obstructive (involve respiratory airways ? increased resistance to air flow
22. Chronic Obstructive Pulmonary Disease (COPD)
Characterized by chronic air flow obstruction in lungs
Reduction in the ratio of forced expiratory volume in the first second to forced vital capacity (FEV1/FVC)
Symptoms:
Difficulty breathing, wheezing, cough, etc�
Increase rapidly in >50 years of age, frequent in men
Cause:
Environmental factors and age (also genetic predisposition)
80% of cases is due to cigarette smoking
Two most common types: Emphysema & Chronic bronchitis
23. Emphysema
Excessive air accumulates in lungs as they lose their ability to ventilate properly
More prevalent in older people
Gradual development in response to smoking, bronchitis, pulmonary irritants
Mechanism
Chronic irritation, smoking, infections ? paralyze & deteriorate mucus membrane cilia ? excessive mucus production w/in airways to the lungs ? persistent cough
? collapse of airways ? hinders air flow through lungs ? air becomes trapped in alveoli
Trapped air ? alveoli remain inflated ? expiration (normally passive action) requires muscular resistance ? significant energy needed to exhale ? development of Barrel Chest
24. Over-inflated alveoli destroy alveoli�s wall ? replaced by fibrous tissue ? hinder gaseous exchange
Early stages: gaseous exchange fairly adequate ? no cyanosis
Later stages: great reduction in area where gas exchange occurs ? cyanosis even w/ mild physical effort
Patients often have low maximum breathing capacity and high residual air volume
The disease can not be reversed and gradually worsens
Therapy: positive-pressure oxygen therapy to force O2 into alveoli
Emphysema puts extra load on heart (attempts to pump more blood into lungs to compensate for O2 deficiency)
Patients suffering from emphysema die from heart failure
26. Dirty lung of an Emphysema (smoking) patient
27. Bronchitis
Acute or chronic inflammation of the bronchial tree
Caused by bacterial infection or by irritants (smoke in inhaled air)
Chronic bronchitis is due to long-term exposure to environmental insults ? more common in elderly
Similar to emphysema airway irritation responds by mucus production
In severe cases, mucus membrane becomes swollen and partially obstruct airway ? severe hindrance of gas exchange ? cyanosis
Excess mucus buildup is removed by persistent coughing
28. Pneumonia
Inflammation of the lower airways of the lungs
Symptoms: Fever, cough, sputum production (not restricted to older individuals)
Classification (due to variability in causative agents):
Community acquired: viruses (influenza) or pneumococcus
Hospital acquired: gram negative bacilli (E. Coli) or Enterobacter
Aspiration pneumonia: inhalation of foods or foreign bodies that obstruct bronchus
causes lung collapse, fluid accumulation, infection
More common in older (bedridden) individuals
31. Tuberculosis
Caused by mycobacterium tuberculosis ; enters body with inspired air ? lung tuberculosis is the most common form
Symptoms: early (subtle) weight loss, fever, cough
Diagnosis: skin test, chest x-ray, sputum culture
Lung phagocytes ? destroy the bug ? alive bacteria are walled off in small or calcified nodules (Tubercle)
Evading bacteria ? spread ? lung tissue replaced by fibrous tissue ? reduced vital capacity and difficulty breathing
Antibiotics harnessed TB till mid-80s ? resurgence due to AIDS
Role of immune system in controlling outward signs of the disease
Dormancy ? impaired immune system ? Reactivation tuberculosis
33. Pulmonary Embolism
Ambolus: blood clot or foreign objects that flows freely w/in blood vessels
Can reach vessels with small diameter, can not pass through them ? partial or complete block ? reduced blood flow to the tissue ? tissue dies
Pulmonary embolism: a clot that blocks a branch of pulmonary artery
Symptoms: shortness of breath, chest pain, spitting blood, accelerated heart beat and breathing rate, anxiety
Can occur at any age, more common in bedridden older individuals
Immobile patients tend to develop clots in leg veins (low blood flow)
Treatment:
Anticoagulant drugs (streptokinase)