Download
1 / 28
400 likes | 1.1k Views
Dr. Abdelaziz Elamin MD, PhD, FRCPCH Professor of Child Health consultant pediatric endocrinologist Sultan Qaboos University Muscat, Oman. azizmin@hotmail.com. DIABETES INSIPIDUS. DIABETES INSIPIDUS.

E N D
Dr. Abdelaziz Elamin MD, PhD, FRCPCH Professor of Child Health consultant pediatric endocrinologist Sultan Qaboos University Muscat, Oman. azizmin@hotmail.com DIABETES INSIPIDUS
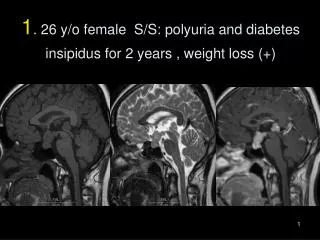
DIABETES INSIPIDUS • DI is a disorder resulting from deficiency of anti-diuretic hormone (ADH) or its action and is characterized by the passage of copious amounts of dilute urine. • It must be differentiated from other polyuric states such as primary polydipsia & osmotic duiresis. Central DI is due to failure of the pituitary gland to secrete adequate ADH.
DIABETES INSIPIDUS /2 • Nephrogenic DI results when the renal tubules of the kidneys fail to respond to circulating ADH. • The resulting renal concentration defect leads to the loss of large volumes of dilute urine. This causes cellular and extracellular dehydration and hypernatremia.
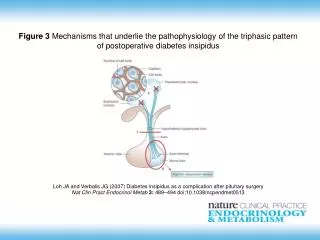
THE POSTERIOR PITUITARY • Is composed of nerve fibers that have their cell bodies in the supraoptic & paraventricular nuclei of the hypothalamus. • The neurosecretory cells in these nuclei synthesize Oxytocin & Vasopressin which pass down the nerve fibres to be stored in & released from the posterior pituitary.
REGULATION OF ADH SECRETION • ADH RELEASE IS STIMULATED BY: • A PLASMA OSMOLALITY >280 mOsm/l • A FALL IN PLASMA VOLUME • EMOTIONAL FACTORS & STRESS • SLEEP • OTHER FACTORS
Other ADH Stimulants • CHOLINERGIC STIMULATION • a-ADRENERGIC STIMULATION • ANGIOTENSIN II • PROSTAGLANDIN E • OPIATES • NICOTINE • HISTAMINE • ETHER • PHENOBARBITONE
ADH SECRETION IS INHIBITED BY: • ALCOHOL • OROPHARYNGEAL WATER REFLEX • b-DRENERGIC STIMULANTS • ATRIAL NATRIURETIC FACTOR (ANF) • PHENYTOIN
ADH • THE SUPRAOPTIC NUCLEUS (SON) IS RESPONSIBLE PREDOMINANTLY FOR THE SYNTHESIS OF VASOPRESSIN WHICH IS THE ADH. • THE CLOSE STRUCTURAL SIMILARITY OF VASOPRESSIN & OXYTOCIN EXPLAINS THE OVERLAP OF THEIR BIOLOGICAL ACTIONS.
ADH (2) • ADH IS AN OCTAPEPTIDE LIKE OXYTOCIN. • THE ARGININE VASOPRESSIN IS ADH IN MAN AND OTHER MAMMALS APART FROM THE PIG & THE HIPPOPOTAMUS WHERE LYSINE VASOPRESSIN IS THE ADH.
FUNCTION OF ADH • PRIMARY EFFECT OF ADH IS ON THE CELLS OF THE DISTAL TUBULES & COLLECTING DUCTS OF THE KIDNEY PROMOTING REABSORPTION OF WATER. • THIS ACTION IS MEDIATED VIA V2-RECEPTORS THROUGH ACTIVATION OF cAMP AND FORMATION OF A SPECIFIC PROTEIN KNOWN AS AQUAPORIN.
Actions of ADH (2) • Beside water, AVP enhances reabsorption of urea increasing tonicity of the renal medulla allowing more water to be re-absorbed. • Acting on v1-receptors in peripheral vessels AVP causes vaso-constriction & BP. Normally this is balanced by its inhibitory effect on sympathetic cardiac stimuli causing bradycardia
Actions of ADH (3) • DURING HYPOVOLEMIA HIGH PLASMA LEVELS OF AVP HELP MAINTAIN TISSUE PERFUSSION. • A LESSER SECONDARY EFFECT THAT IS MEDIATED VIA V2 NON-RENAL RECEPTORS IS STIMULATION OF SYNTHESIS & RELEASE OF FACTOR VIII & VON WILLEBRAND FACTOR.
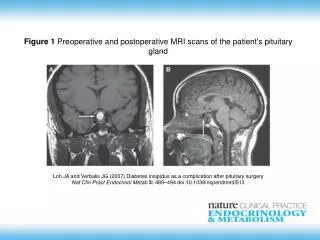
CAUSES OF CENTRAL DI • IDIOPATHIC (30% OF CASES) • SUPRASELLAR TUMOURS (30% OF CASES) • INFECTIONS (ENCEPHALITIS, TB, etc) • NON-INFECTIOUS GRANULOMA (SARCOID, HAND-SCHULLER CHRISTIAN DISEASE • TRAUMA OR SKULL SURGERY • LEUKAEMIA
CAUSES OF CENTRAL DI (2) • AUTOIMMUNE ASSOCIATED WITH THYROIDITIS • FAMILIAL: 2 TYPES AD & X-LINKED INHERITANCE • WOLFRAM SYNDROME (ALSO KNOWN AS DIDMOAD SYNDROME) CHARACTERIZED BY DI, DM, NERVE DEAFNESS AND OPTICATROPHY.
CAUSES OF NEPHROGENIC DI • PRIMARY FAMILIAL:X-LINKED RECESSIVE THAT IS SEVERE IN BOYS & MILD IN GIRLS • SECONDARYTO: • CHRONIC PYELONEPHRITIS • HYPOKALEMIA • HYPERCALCEMIA • SICKLE CELL DISEASE • PROTEIN DEPRIVATION
CAUSES OF NEPHROGENIC DI/2 • SECONDARY CAUSES continued: • AMYLOIDOSIS • OTHER RENAL DISEASES (chronic renal failure, obstructive uropathy, polycystic disease) • SJOGREN SYNDROME • DRUGS (Lithium, Colchicine, Fluoride, Cidofovir, Demeclocycline, Methoyflurane)
CLINICAL FEATURES • POLYURIA, POLYDIPSIA & THIRST • NOCTURIA OR NOCTURNAL ENURESIS • HYPERNATREMIC DEHYDRATION • ANOREXIA, CONSTIPATION & FTT • HYPERTHERMIA & LACK OF SWEATING • SYMPTOMS OF UNDERLYING CAUSE
COMPLICATIONS • HYPERNATREMIC DEHYDRATION & ITS NEUROLOGICAL SEQUELEA • GROWTH RETARDATION • HYDRONEPHROSIS (DUE TO EXCESSIVE URINE OUTPUT)
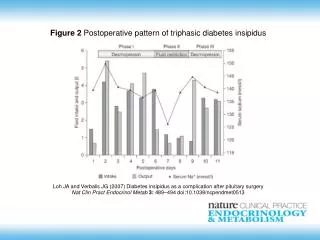
DIAGNOSTIC WORKUP • CAREFUL HISTORY & EXAMINATION DOCUMENT PRESENCE OF POLYURIA (USUALLY 4-15 L/24h) • PRACTICALLY SMILTANEOUS MEASUREMENT OF PLASMA & URINE OSMOLALTY ESTABLISH THE DIAGNOSIS IN MOST CHILDREN WITH SEVERE DI MAKING A WATER DEPRIVATION TEST UNNECESSARY
DIAGNOSTIC WORKUP (2) • URINALYSIS & MICROSCOPY TOGETHER WITH PLASMA ELECTROLYTES HELP EXCLUDE MOST OF THE CAUSES OF POLYURIA • IN A NORMAL WELL HYDRATED SUBJECT PLASMA OSMOLALITY IS <290 mOsml/l AND URINE OSMOLALITY IS 300-450 mOsmol/l
DIAGNOSTIC WORKUP (3) • IN PATIENTS WITH DI & FREE EXCESS TO WATER PLASMA OSMOLALITY IS >295 mOsmol/l & URINE OSOLALITY IS 50-150 mOsmol/l. • IN PATIENTS WITH DI & FREE EXCESS TO WATER PLASMA OSMOLALITY IS >295 mOsmol/l & URINE OSOLALITY IS 50-150 mOsmol/l.
WATER DEPRIVATION TEST • WATER DEPRIVATION TEST IS NEEDED FOR PATIENTS WITH PARTIAL AVP DEFICIENCY & ALSO TO DIFFERENTIATE DI FROM PRIMARY POLYDIPSIA WHICH IS VERY RARE IN CHILDREN
WATER DEPRIVATION TEST (2) • SHOULD BE DONE IN THE MORNING UNDER OBSERVATION • 8 HOURS FAST IS ENOUGH FOR CHILDREN • WEIGH THE CHILD HOURLY AND MEASURE PLASMA & URINE OSMOLALITY EVERY 2 HOURS • IN NORMAL SUBJECTS PLASMA OSMOLALITY HARDLY RISES (< 300) BUT THE URINE OUTPUT IS REDUCED & ITS OSMOLALITY RISES (800-1200)
WATER DEPRIVATION TEST (3) • PATIENTS WITH PRIMARY POLYDIPSIA START WITH LOW NORMAL PLASMA OSMOLALITY (280) BUT URINE/PLASMA OSMOLALITY RATIO RISES TO >2 AFTER DEHYDRATION. • IN PATIENTS WITH DI THE PLASMA BUT NOT THE URINE OSMOLALITY RISES AND U/P OSMOLALITY RATIO REMAINS < 1.5
WATER DEPRIVATION TEST (4) • AT THE END OF THE TEST, ADH IS GIVEN (20 mg DDAVP INTRNASALLY OR 2 mg I.M.) AND FLUID INTAKE ALLOWED. • CONCENTRATION OF THE DILUTE URINE CONFIRMS CENTRAL DI AND FAILURE SUGGEST NEPHROGENIC CAUSES
TREATMENT • DESMOPRESSIN (DDAVP) A SYNTHETIC ANALOG IS SUPERIOR TO NATIVE AVP BECAUSE: • IT HAS LONGER DURATION OF ACTION (8-10 h vs 2-3 h) • MORE POTENT • ITS ANTIDIURETIC ACTIVITY IS 3000 TIMES GREATER THAN ITS PRESSOR ACTIVITY
DDAVP • USUALLY GIVEN INTRANASALLY BUT CAN BE GIVEN ORALLY OR I.M. FOR COMATOSE PATIENTS OR DURING SURGERY. • DDAVP CAN ALSO BE USED IN MILD HAEMOPHILIA OR VON WILLEBRAND DISEASE AND AS TREATMENT FOR NOCTURNAL ENURESIS IN CHILDREN
TREATMENT OF NEPHROGENIC DI • PROVISION OF ADEQUATE FLUIDS & CALORIE • LOW SODIUM DIET • DIURETICS • HIGH DOSE OF DDAVP • CORRECTION OF UNDERLYING CAUSE • DRUGS (Indomethacin, Chlorprooramide, Clofibrate & Carbamazepine)