Download
1 / 20
310 likes | 580 Views
DIABETES INSIPIDUS AND ADIPSIA. JONATHAN D. LEFFERT, MD SEPTEMBER 22, 2004. CASE PRESENTATION.

E N D
DIABETES INSIPIDUS AND ADIPSIA JONATHAN D. LEFFERT, MD SEPTEMBER 22, 2004
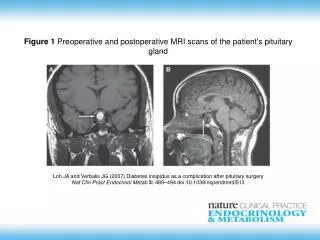
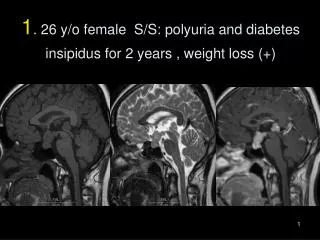
CASE PRESENTATION • N.D. is a 51 yo female who presented initially to Lake Pointe Hospital after suffering the “worst headache of her life”. Neuro evaluation showed some mental status changes but no focal deficits. CT scan of the head showed a subarachnoid hemmorhage. She was care flighted to PHD for further evaluation and treatment.
DIAGNOSTIC STUDIES AND TREATMENT • Cerebral angiography showed 4-5 mm anterior communicating aneurysm which came off the left internal carotid artery. • Surgical clipping of the aneurysm was performed without complication.
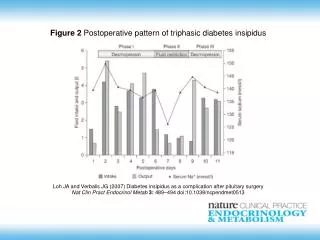
POSTOPERATIVE COMPLICATIONS • On the second hospital day, the patient developed significant polyuria and her serum sodium was 164 with serum osmolality of 326 and urine osmolality of 85 consistent with diabetes insipidus. Pt was still intubated at the time, so IV fluids were increased to keep up with urine output and IV DDAVP was institututed
POSTOPERATIVE COMPLICATIONS • The patient continued to require intermittent DDAVP to maintain her sodium in the normal range, however on Day #4 post op, she abruptly dropped her sodium to 121 with serum osmo of 258 and urine osmo of 611. Her urine volume at this time was in the 2000 cc range daily. This was consistent with SIADH.
POSTOPERATIVE COMPLICATIONS • At this time, her DDAVP was discontinued and her fluids were restricted. By the next day, Postop day # 6, her sodium was back to 149 with serum osmo of 299 and urine osmo of 132 consistent with return of her DI. Her DDAVP was reinstituted and hypotonic saline was started. Throughout this entire period, she never complained of thirst.
FOLLOWUP CARE • N.D. was transferred to the floor and ultimately to rehab. During this time, her sodium fluctuated from 145-155, and urine output was 2000-3000 cc per day. She never complained of thirst, and therefore for her DI, received DDAVP 0.2 mg qhs, and 0.1 mg q am with a fluid prescription of 3000 cc per day.
INCIDENCE OF DI AND ADIPSIA IN SAH • Most common problem is SIADH which occurs in 5-10% of patients with aneurysms • DI is less common at 0.04% • ACA provides vascular supply to region that regulates both thirst and osmoregulated release of AVP • ACOM aneurysms are at increased risk for DI because small perforating branches provide blood supply to the anterior hypothalamus
INCIDENCE OF DI AND SIADH IN SAH • There have been at least 18 reports of ACOM aneurysms with adipsia and DI in the literature. • The intact thirst mechanism prevents the individual with DI from developing significant hypernatremia because of the intense drive to replace free water. • Adipsic DI delays the recognition of DI and increases the risk of life threatening hypernatremia.
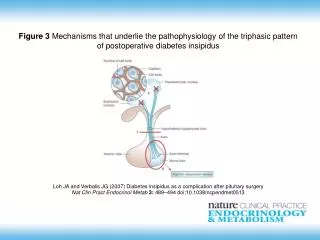
PHYSIOLOGY OF THIRST AND AVP RELEASE • Three mechanisms maintain the plasma sodium and osmolality within a narrow range: the antidiuretic action of AVP on the kidney, normal kidney function and the drive for thirst.
PHYSIOLOGY OF THIRST AND AVP RELEASE • Changes in total body water results in changes in plasma osmolality • Increased plasma osmolality stimulates AVP secretion and thirst. • It is unclear whether AVP release precedes thirst stimulation or if it occurs concurrently.
AVP RELEASE • 1-2% change in osmolality stimulates a release of AVP • AVP secretion is suppressed below 280 • AVP binds to V2 receptor on the renal collecting tubule stimulating intracellular protein kinases which regulate the arrangement of the water channel proteins(aquaphorins). • Water passes from the lumen of the nephron through the aquaphorins in the cells of the collecting duct.
PROTECTION FROM DEHYDRATION • Once the threshold of plasma osmolality of 295 is reached, AVP induced urinary concentration is maximized and increased fluid intake is required. • With free access to water, the thirst mechanism will result in rapid increase in total body water
OSMORECEPTORS , AVP RELEASE AND THIRST • Osmoreceptors which are located in the anterior hypothalamus mediate the effects of increased osmolality on AVP release and thirst • Neural signals from the osmoreceptors project to the supraoptic nucleus where the AVP precursor is synthesized. • Neurons then project to the posterior pituitary where AVP is released.
TYPES OF ADIPSIA • Most patients with ACOM aneurysms have Type C Adipsia which is associated with complete destruction of the osmoreceptors that affect both thirst and AVP release. • The other types of adipsia can differentially affect either one of the two different osmoreceptors
PRESENTATION OF DI • Polyuria, polydipsia with hypotonic urine. Must be differentiated from osmotic diuresis • Urine osmolality of <300 or S.G. <1.010 • Nephrogenic DI can be differentiated on the basis of history and the presence of hypokalemia, hypercalcemia, or exposure to lithium
CENTRAL DI VS. ADIPSIC DI • Those with central DI with intact thirst and access to water, will maintain their plasma osmolality and plasma sodium in the normal range. • In contrast, in adipsic DI, dehydration, hypotension, and altered mental status will occur if fluids are not provided along with DDAVP
TREATMENT OF DI • DDAVP is an analogue AVP that selectively acts at the V2 receptors. • Onset of action can be as soon as 1 hour and duration is between 6-24 hrs. • Different formulations include injection, intranasal, rhinal tube and oral • Dosing varies considerably and each formulation must be titrated individually based upon osmolality and control of polyuria.
TREATMENT OF ADIPSIC DI • Much greater challenge because pt must be prescribed a daily intake of fluids in addition to DDAVP • Close monitoring of weight, urine output and plasma sodium must be done on regular basis to exclude hypernatremia or hyponatremia
FOLLOWUP OF N.D. • Currently at home at night and during day, at Rehab facility. • Sodium has ranged from 135-155 based primarily on her fluid intake • Mental status fluctuates with her Sodium.