Download
1 / 33
330 likes | 496 Views
MRI and CT scanning Statins Antibiotics Coronary artery bypass graft surgery Hip and knee replacement Chemotherapy Radiotherapy Randomised controlled trials Systematic reviews. Great innovations of the first and second healthcare revolution.

E N D
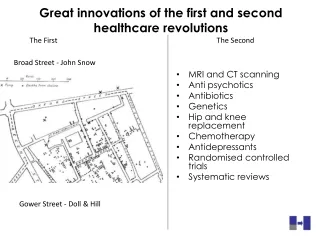
MRI and CT scanning Statins Antibiotics Coronary artery bypass graft surgery Hip and knee replacement Chemotherapy Radiotherapy Randomised controlled trials Systematic reviews Great innovations of the first and second healthcare revolution The First The Second Broad Street - John Snow Gower Street - Doll & Hill
SAFETY - QUALITY FAILURE TO MAXIMISE VALUE INEQUALITIES FAILURE TO PREVENT - At the beginning of C21 5 problems of remain • And there are new challenges • SOCIAL • FINANCIAL • CARBON
High Value High Value High Value Low Value Low Value Added value from doing things right (quality improvement)
High Value High Value High Value Low Value Low Value Added value from doing things right (quality improvement) Added value from doing the right things) making the right decisions
A SYSTEM is a set of activities with a common set of objectives ( also known as a service)A NETWORK is a set of individuals and organisations that deliver the system’s objectives ( a team is a set of individuals or departments within one organisation)A PATHWAY is the route patients usually follow through the network
This is an example of a national service set up as a system
Research Ideas and Information Innovation Patient Clinician Knowledge System Information Ideas and Information
HIERARCHY NETWORK
A SYSTEM is a set of activities with a common set of objectives ( also known as a service)A NETWORK is a set of individuals and organisations that deliver the system’s objectives ( a team is a set of individuals or departments within one organisation)A PATHWAY is the route patients usually follow through the network A PROGRAMME is a set of systems with a common knowledge base and a common budget
Cancers Respiratory Gastro- intestinal
Mental Health Cancers Respiratory Gastro- intestinal
Mental Health Cancers Respiratory PEOPLE WITH MORE THAN ONE DIAGNOSIS Gastro- intestinal
Children Medically Unexplained Physical Symptoms Older People With four or more diagnoses Homeless people
Within programme marginal analysis Breast bowel cancer lung cardiac mental health
Breast bowel cancer lung cardiac mental health Within System marginal analysis Smoking Cessation Chemo PET Scans
Dr Jones is a rheumatologist in the Brighton and Sussex Hosptial Trust and last year she saw 846 people with Rheumatoid Arthritis and tried to provide evidence based, patient centred care, and to improve effectiveness, productivity and safety
Dr Jones estimated that there are 2138 people with Rheumatoid disease in East Sussex and a population based audit showed that there were 200 people who were not referred who would benefit
Dr Jones, the co-ordinator of the Sussex Rheumatoid Clinical Network and Service now sees 1043 patients all of whom benefit
Dr Jones, the co-ordinator of the Sussex Rheumatoid Clinical Network and Service has responsibility, authority and resources ( 2 pa’s and support ) for Network development Localisation of the Map of Medicine Quality of patient information Professional development of generalists, physios and pharmacists www.nhs.uk/sussex/rheumatoid Production of the Annual Report of the service She is keen to improve her performance from being 37th out of the 106 Rheumatoid Arthritis services
Musculoskeletal programme- variation in knee replacement costs Primary knee replacements cost £5,808. There is a 4-fold variation in expenditure between PCTs (adjusting for age, sex and need). The coefficient of variation is 21.0%. (This takes into account all PCTs, not just the top and bottom PCTs.) The potential savings are £39M (if PCTs with rates higher than the median reduced to this level). London
‘if success is truly defined as achieving population based improvement, why not alignat least a proportion of rewards with achieving this overall aim?Mandel k e (2010)aligning rewards with large scale improvementjama 303;663-4
we must ensure that allstudents acquire a basic understandingof how medical care isfinanced, where national healthcare policies come from, and thepolitics that shape financing andworkforce choices.Cost Consciousness in Patient Care — What Is MedicalEducation’s Responsibility?Molly Cooke, M.D.n engl j med 362;14 nejm.org april 8, 2010 1253
‘ the shift in England from the traditional ‘knightly’ policy paradigm to provider challenge through a regime that inflicted public reputational challenge on organizations that failed to achieve national targets, worked.’ Bevan G (2010) Impact of devolution on health care in the UK; provider challenge in England and provider capture in Wales, Scotland and Northern Ireland J health serv res and policy 15; 68-69
The values this patient places on benefits and harms of the options Evidence Choice Decision The clinical condition of this patient; other diagnoses and risk factors
Citizens Information Knowledge Technology The Drivers of the Third Industrial Revolution (Manuel Castells)