Download
1 / 12
120 likes | 487 Views
Physician Compensation Model Tool for Change. 10th Annual Region IX Management Training Conference November 7, 2003 Presented By Matthew M. King, MD Medical Director Clinica Adelante, Inc. Struggling vs Model CHCs What’s the differences?. Cohesive, Experienced Management Shared Vision

E N D
Physician Compensation Model Tool for Change 10th Annual Region IX Management Training Conference November 7, 2003 Presented By Matthew M. King, MD Medical Director Clinica Adelante, Inc.
Struggling vs Model CHCsWhat’s the differences? • Cohesive, Experienced Management • Shared Vision • Tend to be Larger in Size • Medical Director Active Administratively • Sound Business Principles • Emphasis on Quality • Excellent Salaries and Benefits • Know How to “Find the $$”
Emerging Clinics • How do struggling clinics make the transition? Just C H A N G E!!
Physician Incentives Are Your Most Powerful Tool For Change • Traditionally Cited Benefits of Physician Incentive Plans: • Increased Productivity • Improved Retention and Recruitment • More Competitive Salaries
Other (less obvious)Benefits • Aligns Clinical and Administrative Objectives • Incentives must be chosen, expressed clearly and the results accurately captured. • Forces Administrative Excellence • Must prioritize clinic objectives • Must capture important data accurately, quickly and on an ongoing basis. • Reconnects the administration with the clinical operations
Other Benefits(continued) • Mandates Clinic Reengineering • Clinicians expect enough patients to make their bonuses resulting in a focus on customer service, improved physician support and improved processes. • Clinical objectives usually include quality. • Results in Improved Infrastructure • Accurate data capture assumes a greater importance.
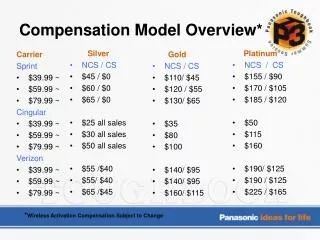
Original Homegrown Physician Incentive Plan Notes: OK to Bonus with Encounters, RVUs, or Both. Bonuses are paid monthly.
Salary Information for Arizona CHC Clinicians Family Practice Salary Standards LowHighAverage $109,990 $ 168,000 $122,268
New Homegrown Physician Incentive Plan Notes: Base numbers are not clinic expectations but numbers to base bonus productivity calculations from. ALL Providers are expected to make bonuses. Quality Bonus are not awarded unless a productivity bonus is earned. All productivity bonuses are 3%, 10% or 20% of Base Number: either Encounter or RVU’s
New Homegrown Physician Incentive Plan (continued) Notes: Quality Indicators (QI) will usually be at least 6 months duration but may be changed every 2 months. Any anticipated changes will be announced no less than 2 months before first pay-outs. QI’s may be provider specific, site specific, global or specialty specific. They may also be based on customer service, patient satisfaction surveys, clinic or community service parameters or other qualitative measures A single QI may be a group of related data or a single parameter. Each Bonus Level will have criteria in addition to the criteria expected on the previous Bonus Level.
Results of Our Incentive Efforts • Purchased an EMR to accurately capture data at point of service. • Formed a reengineering team to improve custom service, minimize system errors and build quality into our routines. • Continued excellent productivity • Improved communication and alignment between administration and clinical staff.
Get Smart . . . Get Started JUST DO IT! • Start Small and Build Slowly • Don’t Wait for Everything to be Right • You Don’t Need Consensus to Move Forward • Leave Yourself a Way Out