Download
1 / 20
200 likes | 606 Views
Predicting the immunogenicity of structural HLA class I epitopes Reyna Goodman. Introduction. Between 5-10% of patients waiting for a renal transplant are classified as highly sensitised (Panel Reactive Activity ≥85% IgG)

E N D
Predicting the immunogenicity of structural HLA class I epitopesReyna Goodman
Introduction • Between 5-10% of patients waiting for a renal transplant are classified as highly sensitised (Panel Reactive Activity ≥85% IgG) • Highly sensitised renal dialysis patients wait longer for a suitable crossmatch negative donor compared to non-sensitised patients • Identification of acceptable HLA mismatches increases the likelihood of transplantation
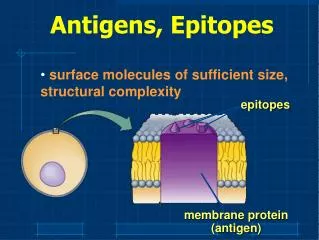
HLA specific antibody screening using single antigen beads • Beads are coated with single HLA specificities • Each bead population has a different ratio of two dyes which allows identification of up to 100 individual HLA specificities • Analysed using a Luminex platform
HLAMatchmaker • A computer algorithm that determines HLA compatibility at a structural level by comparing differences between polymorphic amino acid triplets in the antibody accessible region of the HLA molecule • HLAMatchmaker performs inter-locus and intra-locus comparisons between the patient’s HLA type and each mismatched HLA specificity and calculates the number of amino acid triplet mismatches
Aim • To determine whether HLAMatchmaker could be used to predict the immunogenicity of structural epitopes • comparing acceptable HLA mismatches identified using single antigen HLA specific antibody detection beads with those predicted using the HLAMatchmaker computer algorithm • To identify acceptable HLA mismatches for highly sensitised patients
Patient cohort Of 406 patients on the Addenbrooke’s Hospital renal transplant waiting list, 24 were identified as highly sensitised and selected for study
Data analysis • Single antigen beads detect antibody to 65 individual HLA-A and -B specificities of which 64 are represented in the HLAMatchmaker algorithm • Patient HLA class I types and each mismatched HLA specificity represented on the single antigen beads were entered into the HLAMatchmaker program to determine the number of triplet mismatches • Logistic regression analysis was used to determine the relationship between the detection of antibody using single antigen beads and the number of amino acid triplet mismatches for each HLA specificity determined by HLAMatchmaker
HLA specific antibody screening using single antigen beads • The serum sample with the highest PRA was selected for study • Of 1,451 mismatched HLA specificities, 972 (67%) were antibody positive • A mean of 19 (range 1 - 41) acceptable mismatches were identified for each patient • For 19 patients there were 10 or more acceptable mismatches identified including some common antigens
Presence of antibody for each mismatched HLA specificity categorised by triplet mismatch
Logistic regression analysis of antibody binding to single HLA specificities stratified by number of triplet mismatches % antibody positive 40 20 0 P<0.001 Number of amino acid triplet mismatches
Patient 1 Patient 2 Patient 3 Patient 4 Patient 5 Patient 6 Patient 12 Patient 7 Patient 8 Patient 9 Patient 10 Patient 11 Patient 13 Patient 14 Patient 15 Patient 16 Patient 17 Patient 18 Patient 23 Patient 24 Patient 20 Patient 21 Patient 22 Patient 19 Individual logistic regression analyses of antibody binding to single HLA specificities stratified by number of triplet mismatches Proportion antibody positive Number of triplet mismatches
Conclusions • HLAMatchmaker is an effective tool for predicting the immunogenicity of a particular HLA mismatch • The number and nature of triplet mismatches for a given HLA type correlates with the risk of humoral sensitisation • The presence of a single triplet amino acid mismatch is often sufficient to invoke a strong antibody response • In combination with single antigen beads, acceptable mismatches were identified for highly sensitised patients, increasing access to the donor pool • Goodman et al Transplantation 2006;81:1331-1336
Triplets versus eplets • Examine the extent to which the structural information provided by triplet and eplet epitope analysis of HLA compatibility enables the prediction of: • Acceptable mismatches • Magnitude of the antibody response
Data analysis • Sera obtained from 34 highly sensitised patients were screened using single antigen beads, to determine the presence and magnitude of HLA alloantibody • Patient HLA class I types and each mismatched HLA specificity represented on the single antigen beads were entered into the HLAMatchmaker program to determine the number of triplet and eplet mismatches • A total of 85 sera were screened (median 2 sera per patient, range 1 to 6) and 2,088 mismatched combinations examined • The qualitative and quantitative relationship between alloantibody levels to each HLA specificity and the number of triplet and eplet mismatches was determined
Frequency Frequency 0 50 100 150 200 250 300 0 50 100 150 200 250 300 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 0 1 2 3 4 5 6 7 8 9 10 11 12 13 Triplets Eplets Number of triplet & eplet mismatches present within mismatched HLA specificities P<0.001
Proportion Antibody Positive Proportion Antibody Positive P<0.001 P<0.001 P<0.001 P<0.001 Triplets Eplets Relationship between triplet & eplet mismatches and alloantibody production
Median Fluorescence Intensity Median Fluorescence Intensity Triplets Eplets Relationship between triplet & eplet mismatches and alloantibody levels P>0.001 P>0.001
Conclusions • The number of triplet and eplet mismatches between an alloantigen and the recipient HLA type correlates closely with both the development and strength of an alloantibody response • Eplets offer additional epitope discrimination but do not improve HLA immunogenicity prediction • Self triplets and eplets may form immunogenic epitopes when expressed in a different conformation on mismatched HLA alloantigens
Acknowledgements H&I department Cambridge University Hospitals NHS Foundation Trust, Addenbrooke’s Hospital Dr Craig Taylor Miss Cheryl O’Rourke Mr Tim Key Department of Surgery, University of Cambridge, Addenbrooke’s Hospital Prof J Andrew Bradley Mr Vasilis Kosmoliaptsis Centre for Applied medical statistics, University of Cambridge Mr Andrew Lynch Dr Linda Sharples
Patient follow-up • 5/24 patients transplanted