Download
1 / 75
760 likes | 1.75k Views
The Hand. Bucky Boaz, ARNP-C. Examination of the Upper Extremity. A detailed history should include: Patient’s age Handedness Occupation Hobbies Chief complaint Description of how and when the problem started Duration of symptoms Aggravating and alleviating factors.

E N D
The Hand Bucky Boaz, ARNP-C
Examination of the Upper Extremity • A detailed history should include: • Patient’s age • Handedness • Occupation • Hobbies • Chief complaint • Description of how and when the problem started • Duration of symptoms • Aggravating and alleviating factors
Examination of the Upper Extremity • If an injury is involved: • The environment in which the injury or insult occurred should be determined. • If crush injury, are heat or chemicals involved? • Was the environment clean or dirty? • Past medical history is useful in the presence of systemic conditions that have manifestations in the hand.
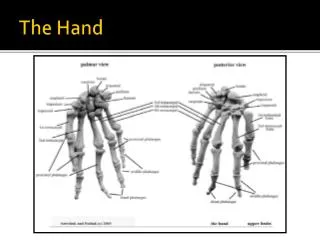
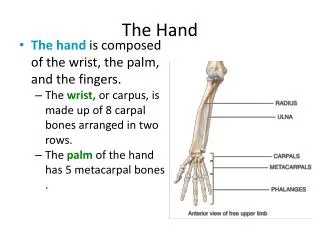
Anatomy Review • Bones • Distal radius and ulna • Carpals metacarpals • Phalanges • Proximal • Middle • Distal
Anatomy Review • Joints • DRUJ • Carpal-Metacarpal • Metacarpal-Phalangeal • Proximal Interphalangeal • Distal Interphalangeal DIP PIP M-P C-M DRUJ
Anatomy Review • Muscles & Tendons • Extrinsic • Flexor tendons • Flexor carpi ulnaris • Flexor carpi radialis • Palmaris longus • Flexor pollicis longus (FPL) • Flexor digitorum profundis (FDP) • Flexor digitorum superficialis (FDS)
Anatomy Review • Muscles & Tendons • Extrinsic • Extensor tendons • Abductor pollicis longus • Extensor pollicis brevis • Extensor carpi radialis longus and brevis • Extensor digitorum • Extensor digiti minimi • Extensor carpi ulnaris
Anatomy Review • Muscles & Tendons • Extrinsic • Extension of MP • Flex of IP • Intrinsic • Abduct and adduct fingers • Flexion of MP • Extension of IP
Anatomy Review • Nerves • Median • Ulnar • Radial
Examination of the Hand and Wrist • Complete exam: • Observation • Palpation • Range of motion • Neurologic testing • Vascular assessment • Stability testing
Observation • Hands at rest • Curved posture • Look for one finger curved • Asymmetry • Color • Spooning or clubbing • Muscle atrophy
Palpation • Lateral epicondyle • Radial head • Groove of ulnar nerve • Olecranon • Lister’s tubercle • Radial/ulna styloid • Snuffbox • Carpals • Metacarpals • Phalanges
Neurologic Testing • Sensory • Light touch – pin prick • Two-point descrimination • Motor • Median • Ulnar • Radial
Neurologic Testing • Motor testing • OK sign • FDP • FDS • FPL
Vascular Examination • Radial artery • Located radial to the FCR • Ulnar artery • Located radial to the FCU • Allen test
Stability Testing • Ulnar collateral ligaments • Radial collateral ligaments • Gamekeeper’s/ skier’s thumb
TAP Special Tests • Finklestein’s test • Froment’s sign • Watson test • Shuck test • Basal joint grind • Compression test • Phalen’s test • Tinel’s sign
Common Traumatic Injuriesof the Hand Bone and Soft Tissue
Considerations on Treating Hand Injuries • Type of injury • The patient • Associated diseases • Socioeconomic factors • Ability to cooperate with treatment plan • Motivation to get well • Managing the patient • Recognizing the injury • Making the proper diagnosis • Initiating the appropriate care plan
Referrals • Emergent referrals • Open fractures • Fractures with neurovascular compromise • Significant soft tissue injury • Irreducible dislocations or fractures with significant deformity
Referrals • Urgent referrals (next day or two) • Closed flexor or extensor tendon injuries • Displaced, angulated, or malrotated closed fractures • Carpal bone and distal radius fractures
History • Complete history • Hand dominance • Occupation • Avocations • Circumstances surrounding the injury • When and where • Mechanism of injury • Location and character of pain • Numbness or tingling
Radiographs • Examine prior to ordering films • Stress views are useful in demonstrating injuries not present on plain views • Occasionally CT scan or MRI are needed to evaluate an injury
Description of Fractures • Be able to accurately describe a radiograph to a colleague • Correct name of bone or joint involved • Open or closed fracture • Intraarticular or extraarticular • Whether the fracture is shortened, displaced, malrotated, or angulated • Fracture pattern
Description of Dislocations • Be able to accurately describe a dislocation • Described with the position of the distal bone relative to the proximal bone • Dorsal vs volar dislocation • Radial vs ulnar dislocation • Can have a combination of two
Complications • By far, the largest potential problem with any hand or wrist injury is stiffness. • Soft tissue complications: • Tendon adhesions • Capsular contractures • Fracture healing time • Hand: 3-4 weeks • Distal radius: 5-7 weeks
Complications • Bony complications: • Malunion • Angulation • Malrotation • Shortening • Intra-articular step-off • Nonunion is uncommon in hand or wrist
Fractures of the Distal Phalanx • The distal phalanx is the most common fracture in the hand, accounting for approximately 50% of hand fractures
Fractures of the Distal Phalanx • Applied Anatomy • Extensor and flexor tendons insert into the base of the distal phalanx • Routinely not a deforming fracture
Fractures of the Distal Phalanx • Mechanism of Injury • Crush injury • Sudden extension against a flexed finger (rugger jersey) • Sudden flexion against an extended finger (baseball hitting end of extended finger)
Associated Injuries Nailbed lacerations Nail plate avulsion Skin lacerations Subungal hematoma History and Physical Exam Check both flexor and extensor function Document sensory exam Fractures of the Distal Phalanx
Radiographs 2 – 3 views to look for fracture Use hot light if needed Classification Longitudinal Transverse comminuted Treatment Non-displaced or minimally displaced can use variety of splints Immobilize the DIP only Reduce displaced fractures Open wounds may need more definitive treatment Fractures of the Distal Phalanx
Outcomes Cold intolerance Tip sensitivity Stiffness Nailplate irregularities When to refer Open fractures in need of nail bed repair Large skin loss Suspected flexor or extensor tendon involvement Fractures of the Distal Phalanx
Nailbed Injury • Nailbed lacerations need to be repaired • Use 6-0 absorbable to repair matrix • Prevents nail growth problems • Reinsert nail and secure
Subungual Hematoma • Results from blunt trauma to nail • Very painful • Relieved by • Cautery • Heated paperclip • 18g needle
Subungual Hematoma • Clean with alcohol • Instrument of choice • Pierce nail • Gauze for 24 hours
Mallet Fingers(soft tissue and bony) • Applied Anatomy • Terminal extensor tendon inserts into the dorsum of the distal phalanx • Mechanism of injury • Occurs with a sudden flexion force against an extended digit • Results in flexion deformity of the DIP joint
Mallet Fingers(soft tissue and bony) • History and Physical Exam • Pain and deformity of the DIP joint after bumping the end of the finger • Inability to straighten the end joint • Test for tendon function
Mallet Fingers(soft tissue and bony) • Radiographs • 2 views looking for dorsal avulsion fragment • May be negative • Classification • Soft tissue (- x-ray) • Bony (+ x-ray) • Fleck • Dorsal articular piece • Subluxation of DIP joint
Mallet Fingers(soft tissue and bony) • Treatment • Closed reduction • Continuously splint DIP in full extension for 6 to 10 weeks • Only immobilize the DIP • Acceptable results may still be obtained with continuous extension splinting if it is as long as 2-3 months after initial trauma
Flexor Tendon Avulsion • Applied Anatomy • Flexor digitorum profundus tendon inserts into the base of the distal phalanx
Flexor Tendon Avulsion • Mechanism of Injury • Hyperextension against a flexed DIP joint • Relatively uncommon, but devastating is missed • Ring finger most commonly involved
Flexor Tendon Avulsion • Associated injuries • None • History and Physical Exam • Pain on volar surface of digit • May extend into palm with eccymosis • Cannot flex tip • Resting hand has extension of DIP joint • No active flexion
Flexor Tendon Avulsion • Radiographs • DIP to look for avulsion, but also hand to look for retracted segment • Most are normal • Classification • Pure tendon avulsion • Bony avulsion
Treatment Should be splinted and referred in a semi-urgent fashion Surgery is required Outcomes Results correlate with delay in treatment Early do well Postoperative hand therapy is important Flexor Tendon Avulsion
Middle and Proximal Phalangeal Fractures • Applied Anatomy • The central slip inserts into the proximal dorsal middle phalanx • The flexor digitorum superficialis (FDS) inserts into each side of the base of the middle phalanx
Middle and Proximal Phalangeal Fractures • Applied Anatomy • Intrinsic muscles of the hand act to flex the MCP joints and extend the PIP and DIP through the actions of the lateral bands
Mechanism of Injury Direct blow to the digit or a twisting injury Associated Injuries Open injuries Lacerations to tendons or neurovascular bundles Important to evaluate for DIP injuries History and Physical Exam Evaluate for malrotation Subtle fractures on x-ray can have significant malrotation when flexed Middle and Proximal Phalangeal Fractures
Middle and Proximal Phalangeal Fractures • Radiographs • 3 views • Evaluate joint proximal and distal • Spiral fracture may appear on only 1 view • Classification
Middle and Proximal Phalangeal Fractures • Treatment • Most can be treated non-surgically • Protect range of motion • Buddy tape • What to refer • Displaced, malrotated, joint involvement • Comminuted, spiral, and oblique are unstable • Stable nondisplaced • Splint 8-10 days followed by buddy tape • Follow-up x-ray 8-10 days to ensure no displacement