Download
1 / 24
260 likes | 738 Views
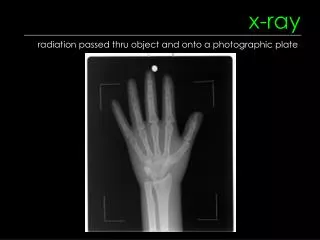
X-ray Diagnosis of Foreign Bodies . Esophageal Foreign Bodies. The easy stuff. Coin in esophagus Model VC-10 in upper esophagus. Patient had tried to conceal the trinket by swallowing it . . A little harder to see. Impacted chicken bone. Food or true foreign bodies

E N D
Esophageal Foreign Bodies The easy stuff
Coin in esophagus Model VC-10 in upper esophagus. Patient had tried to conceal the trinket by swallowing it.
Food or true foreign bodies Chicken bones (opaque), fish bones (non-opaque) Coins, toy trucks Most often they impact just below cricopharyngeous (70%) Another 20% impact at the level of the aortic arch Another 10% at EG junction Once past the esophagus, most foreign bodies will pass through the GI tract Clinical findings of an impacted esophageal foreign body Dysphagia and odynophagia most commonly Even if FB passes, many complain of pain referable to cervical esophagus Always check for lead lines in children Chicken bones are usually opaque Fish bones contain less calcium and usually are not Esophageal Foreign Bodies
Esophageal Foreign Bodies Plain films usually do not demonstrate the FB but are still obtained first If negative, then either contrast esophagram or CT if high index of suspicion Treatment Removal is most often performed using endoscopy Temporization and surgery are other options An ingested button battery lodged in esophagus must be removed immediately Complications of an impacted foreign body Perforation Longer the FB remains impacted (>24hrs), higher incidence of perforation Stricture Diverticulum formation
Further on down An 11-month-old girl History of ingesting a metallic object used for fishing, 15 days prior Fever, vomiting, constipation for 3 days, with convulsions. Absence of meningeal signs or neurological deficits. PE: She had normal fundus, CSF, total and differential leukocyte counts and microcytic hypochromic anemia (Hb 8 g/dL)
9-month-old girl, previously healthy, presented with a history of 1 day with fever, productive coughing and short breath.
17 mth old with a one-hour history of noisy, abnormal breathing after a choking episode while eating a chocolate bar
Foreign body aspiration 75% of all cases children less than 3 years of age. 6-17% of airway foreign bodies are radio-opaque. Peanuts most common. Respiratory symptoms may be produced by an object lodged anywhere in the airway, from the hypopharynx to a segmental bronchus. Presents with: Acute respiratory distress days or months after the aspiration episode. Suggestive history, acute episode of paroxysmal cough, cyanosis, choking, and dyspnea. Triad of coughing, wheezing, and decreased or absent breath sounds is present in only about 40% of cases. Other suggestive physical exam findings are stridor, tachypnea, retractions, rales, and fever. They are often misdiagnosed as croup, asthma, pneumonia, or bronchitis Many go undiagnosed for long periods of time due to lack of radiographic findings Diagnosis: Start with AP and lateral Lateral decubitus and expiratory films can help diagnose air trapping High clinical suspicion with negative films should still indicate need for rigid bronchoscopy
20 year old man referred for removal of a bullet impacted in his left maxillary antrum after walking into the hospital. There was an old land dispute as a result of which an altercation took place, and the patient was hit by his adversary from a distance of around 4 m.
This patient had a penetrating eye injury from a metal fragment while hammering metal on metal without safety glasses. Screenings are done daily for MRI