Download
1 / 36
1.64k likes | 5.8k Views
TRIAGE. Lee Wallis Senior Lecturer Division of Emergency Medicine, UCT/SU. Triage. Background Cape Triage Group Cape Triage Score Development The CTS Validation South African Triage Score EWS in children. Triage. French verb trier To sieve / to sort Medically:

E N D
TRIAGE Lee Wallis Senior Lecturer Division of Emergency Medicine, UCT/SU
Triage • Background • Cape Triage Group • Cape Triage Score • Development • The CTS • Validation • South African Triage Score • EWS in children
Triage • French verb trier • To sieve / to sort • Medically: • The process of applying medical priority to patients to do the most for the most
History of triage • Baron Dominique Jean Larré • Napoleon’s surgeon • Changed the treatment of injured soldiers • Least injured first, return to war • Little improvement until Vietnam • Military now use standard civilian priorities • Triage common to EDs in West for 20+ years
Triage tools • Discriminators: • Demographics • Old or young triaged out • Mechanism of injury • Only for trauma • Anatomy • Dependent upon examination – time consuming • Physiology • Most reliable • Intended use: • Hospital vs Pre-hospital • Day-to-day vs MCI • Trauma vs Other • Adult vs Child
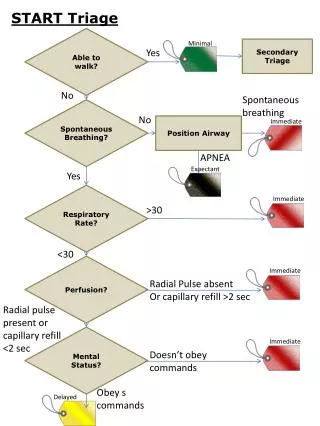
MCI Pre-hospital triage • Do the most for the most • Try to pick out sickest first • Theoretical evidence for leaving these • Easy to learn & use • Close to daily practice • Physiologic most common • Triage sieve, Triage sort, START, Careflight etc • Paediatric Triage Tape
MCI Hospital triage • Triage Sort • RR 0-4 • SBP 0-4 • GCS 0-4 • Total 0-12 • P3 – 12 • P2 – 11 • P1 - other • + Basic Anatomical information
Daily Pre-hospital triage • Often not done • When done - trauma only • TS, RTS, TRTS, PHI, CRAMS, ACS TTC, etc • Children – PTS, adult tools • Physiologically incorrect • Most used to identify need for Trauma Centre care (USA)
Hospital triage - subjective • Senior doctor or nurse • Front door of unit • Eyeball • Gut-feel • Accuracy as low as 35% • Poorly reproducible • 24 / 7 coverage
Hospital triage - objective • MCI – triage sort or similar • Day-to-day • Manchester triage, CTS, ATAS, ESI, PTS • Complicated, time consuming, training implications, senior staff
Cape Triage Group • Convened Jan 2004 • Joint division of Emergency medicine, UCT / SU • Jan 2004 • 32 registrars, 5 waiting posts • Dip PEC, MPhil, MSC, MMed / FCEM • Private & Public • Pre-hospital & hospital • Doctors, nurses, paramedics • 1 speech therapist….
CTG: objectives • Saw the need for triage in W Cape (SA) setting • Develop a tool for hospital EU use • Pre-hospital triage • Not a MCI tool
CTS: staffing considerations Doctors and nurses per 100,000 population per annum for selected countries
CTS: development • Look at other countries’ tools • Look at other options • EWS • Derivation phase • Validation phase
CTS: Priorities • 5 colours • Red Immediate • Orange 10 mins • Yellow 60 mins • Green 4 hours • Blue Dead
CTS: the basics • 2 part tool • TEWS • Discriminators • 3 versions • Adult, Child, Infant • 5 colours
CTS: TEWS • Triage Early Warning Score • From MEWS – UK ICU outreach program • MEWS reduced ICU admission and mortality / LoS • Minor modifications to adult version = TEWS
CTS: adult • TEWS Derivation: from MEWS • Discriminators: committee consensus • Validation • 1500 GF Jooste, 2000 Mediclinic, 12,000 CHC EUs • 2 MPhils
CTS: child & infant • TEWS Derivation: • 1500 healthy school children • 4000 injured children RXH TU • Discriminators: committee consensus • Validation • 8000 children at CHC EUs • Age, height, weight related vital signs • Logistic regression vs neural nets • PhD
Step 1 Measure vital signs and document the findings Step 3 Calculate the TEWS and document the total value Step 4 Match the score to the list and observe the discriminator list for issues not picked up by the TEWS Step 5 Document the triage code and act accordingly CTS: step by step Step 2 Take a brief history directed at the main complaint and document this
Example • 10 year old, electrical burn • Walking (0) RR 24 (1) HR 110 (1) SBP 115 (0) Temp 37 (0) alert (0) trauma (1) • TEWS total = 3 • YELLOW
Discriminators: Adult • Final Triage • ORANGE
CTS: management aids • Series of management pointers • Including: • Diabetes – test glucose • Low temp – blankets • Chest pain – ECG • Aimed at ENA
CTS: benefits • GF Jooste, 4 CHCs: • Reduced waiting times • 590 mins mean, to 30 mins red, 60 orange, 400 green • Decreased EU length of stay • Improved patient flow, decreased overcrowding in EU • Reduction in mortality 2% to 0.7% • Morbidity? • Improved patient and health provider satisfaction
CTS: validity • Overtriage, undertriage • What should a triage tool identify? • Injury severity • Resource usage • Death / High care / Admission • Urgency of Intervention
CTS: Implementation • 1 Jan roll out W Cape • All EUs • Primary Care • Secondary & tertiary care • DoH funded and supported • Intensive training program • Educational materials • Posters, keycards, patient leaflets
Future developments: CTS • 1 year M&E manager • Audits • QA • Performance indicator thresholds • CTS living tool • Modify as needed • Keep same format
Future developments: SATS • CTS taken on by 4 provinces so far • Call for SA Triage Group • First meet June 2006, Durban • Represent all provinces • Develop a SATS • Based on CTS
Future developments: EWS • MEWS part of TEWS for in-patient monitoring • Mortality and morbidity benefit, LoS reduction • Validate child & infant versions • Funding for age – group specific EWS from UK