Download
1 / 84
950 likes | 1.81k Views
Triage. Instructor Name: Title: Unit:. Triage – from the French sort. In casualty management sorting of a large number of injured personnel is the 1 st stage in establishing order Triage sets the stage for treatment and eventuates in transport of the injured.

E N D
Triage Instructor Name: Title: Unit:
Triage – from the French sort • In casualty management sorting of a large number of injured personnel is the 1st stage in establishing order • Triage sets the stage for treatment and eventuates in transport of the injured
Triage is not to be considered with finality • Triage categories change based upon • Number of injured • Available resources • Nature and extent of injuries(s) • State of hostile threat
Number of patients Extent of resources Condition of patient Gets better Gets worse Transport arrives Things change
If you have only 1 patient • That patient is Pri 1 Immediate regardless of anything else • There is no real need for triage • Once this number increases, the need for triage arises
Categories • Immediate • Threat to life/limb • A lightly injured is immediate if he can be returned to duty with immediate simple management
Urgent • Patient is at risk if treatment or transportation is delayed unreasonably
Delayed • No risk to life or consequence if more definitive care is not rendered quickly
Expectant • Regardless of the level of care rendered, patient is likely to expire • Tough call to make for unit personnel
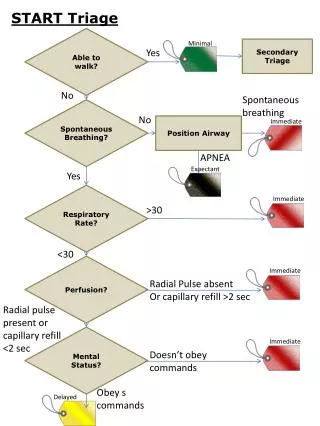
START – triage technique • Simple treat/triage and rapid transport • All of you within the sound of my voice • Move towards me • Doesn’t work well in no/low light or excess noise
Military Triage COL Cliff Cloonan Assistant Professor Military & Emergency Medicine Department Instructor Name: Title: Unit:
Triage • Objectives – Upon completion of this block of instruction the student will be able to:
Triage • Definition – • “To Sort” • From the French word, “trier” • Has been defined as “doing the greatest good for the greatest number” BUT triage is simply a sorting PROCESS that when applied creates a situation that allows for “doing the greatest good for the greatest number”
Triage • What are the OBJECTIVES of doing Triage? • Rapid sorting of the more serious patients from those less serious to facilitate the rapid care of the more serious patients • When problems exceed resources, triage should facilitate “doing the greatest good for the greatest number” • Bring order to chaos thus facilitating the care of all patients
Triage • What is the PROCESS? • Sorting into categories for evacuation and treatment • What are the DECISIONS? • How will the patients be sorted – who goes in which category? • What will be done to/with the patients when sorted? • What factors AFFECT/CHANGE the decisions? • Resources • Circumstances
Sorting Patients “Normal” Triage in an ED TRIAGE - A CONTINUUM Triage in A MASCAL Situation Triage • Special Situations • Persisting threat to providers/patients • “Reverse” Triage Situation
“Normal” Triage in an ED TRIAGE - A CONTINUUM Triage in A MASCAL Situation
Triage • “Military” Disasters Occur In Civilian Settings
Triage • And… “Civilian” disasters occur in military settings
Truck Accident on Pipeline Rd Saudi Arabia – Desert Shield
Resource Modifiers (Manpower, Equipment, Expendables, Time) Disease Process Modifiers (Illness, Injury, NBC, etc) Triage INPUT (Patients to be sorted) OUTPUT (Sorted Patients) Immediate Delayed Minimal Expectant Situation Modifiers (Risk, Weather, MET-T, Combat Situation, etc…) Evacuation Modifiers (Assets, Distance, Threat)
Triage • Military vs. Civilian – Are there differences? • Continuing risk to medical care providers • Can occur in both situations • More common in combat/military triage • Resource limited • Can occur in both situations • More common in combat/military triage • “Reverse” Triage Situation • Care provided first to those who when treated can be quickly returned to duty • Usually only in a military situation but could occur in a civilian MASCAL situation (when “Group” survival is at stake)
Civil War Casualty Collection Point
Civil War Casualty Collection Point and Treatment Station
Vietnam – Mass Heat Casualties
TRIAGE - A DYNAMIC NOT A STATIC PROCESS
WITHIN THE MILITARY ECHELONED MEDICAL CARE SYSTEM, TRIAGE OF CASUALTIES OCCURS (OR SHOULD), AT A MINIMUM, AT EVERY ECHELON
MILITARY TRIAGE OFTEN INCLUDES, BUT IS MORE THAN, MEDICAL PRIORITIZATION
APPROPRIATE MEDICAL PRIORITIZATION AND TREATMENT OF INJURIES IN A SINGLE PATIENT IS THE GOAL OF ADVANCED TRAUMA LIFE SUPPORT TRAINING
What is the Priority Injury? What is the Triage Category? What is the Evac Priority? RPG Wound Right Knee - Somalia
Burn Victim - Kosovo What is the Priority Injury? What is the Triage Category? What is the Evacuation Priority?
Burn Victim - Kosovo
SURGICAL PRIORITIZATION, WHICH, PRIMARILY INVOLVES A DETERMINATION OF OPERATIVE PRIORITY, IS NOT TRIAGE
Triage • Surgical Prioritization Involves - • Recognizing • Which patients require surgery to save life/limb/sight • Knowing • Numbers of OR’s, doctors, nurses, expendables, blood (Resources) each operation requires • Resources (manpower, equip, expendables, blood etc) required to provide post-op care • How long each operation will take (Time as a resource) • The resources that each operation will consume (Must consider manpower as a consumable resource) • Probability of successful surgery
Triage • The Goal of Surgical Prioritization • Selection of cases with the highest probability of success that consume the least amount of resources. • Make a decision - - and go with it! • Once a MASCAL situation has been declared don’t wait for the situation to evolve further before making a decision. • Making decisions is more important than what decisions are made. • Respect the Triage Decision
Grenade • Fragment • Wound – • Perforating • Bowel • ICRC Hospital • Afghanistan
Transverse Abdominal • High Velocity Bullet Wound • ICRC Hospital • Afghanistan
Triage • Triage Categories used in ICRC Hospitals • Category I – Priority for Surgery • Patients who need urgent surgery and who have a good chance of satisfactory recovery • Category II – No Surgery • Patients with wounds so slight that they do not need surgery AND… • Patients who are so severely injured that they are unlikely to survive • Category III – Can Wait For Surgery • Patients who need surgery but not urgently
TRIAGE IN A DISASTER IS A MULTI-DISCIPLINARY PROCESS. IT IS BEST CARRIED OUT BY SOMEONE WHO IS FAMILIAR WITH: • SURGICAL, MEDICAL, AND PSYCHIATRIC EMERGENCIES • ALL THE PRE-HOSPITAL AND HOSPITAL-BASED MEDICAL AND LOGISTICAL RESOURCES NECESSARY TO EVACUATE AND PROVIDE CARE FOR A LARGE NUMBER OF CASUALTIES
BY DEFINITION, TRIAGE IN A DISASTER / MASCAL SITUATION MEANS THAT LESS THAN THE NORMAL STANDARD OF CARE WILL BE PROVIDED FOR MANY PATIENTS.
EXAMPLE: FAILURE TO PROVIDE COMPLETE CONTROL OF THE CERVICAL SPINE IN A PATIENT WITH MULTIPLE BLUNT TRAUMA INJURIES IS CONSIDERED MALPRACTICE
EXAMPLE COMPLETE CERVICAL SPINE IMMOBILIZATION IS VERY TIME AND RESOURCE CONSUMING. THE TIME AND RESOURCES REQUIRED TO STABILIZE A CERVICAL SPINE MAY MEAN THAT OTHERS MAY DIE.
ADHERING TO THE PRINCIPLE OF DOING THE GREATEST GOOD FOR THE GREATEST NUMBER MAY REQUIRE THAT LESS THAN FULL CERVICAL SPINE IMMOBILIZATION BE PERFORMED
REMEMBER IF IT WASN'T ALL "SCREWED" UP IT WOULDN'T BE A DISASTER
REMEMBER NOT ONLY MAY CHANGES IN A PATIENT'S MEDICAL CONDITION RESULT IN A CHANGE IN HIS / HER TRIAGE CATEGORY BUT A CHANGE IN AVAILABLE RESOURCES MAY ALSO RESULT IN A CHANGE IN TRIAGE CATEGORY