Download
1 / 43
450 likes | 1.52k Views
Osteoporosis. Osteoporosis: Scope of the Problem. Osteoporosis is characterized by low bone mass and micro architectural deterioration of bone tissue, leading to bone fragility and an increase risk of fracture 10 million individuals already have osteoporosis. .

E N D
Osteoporosis: Scope of the Problem • Osteoporosis is characterized by low bone mass and micro architectural deterioration of bone tissue, leading to bone fragility and an increase risk of fracture • 10 million individuals already have osteoporosis .
Osteoporosis: Scope of the Problem • 18 million more have low bone mass • One out of two women and one in eight men over 50 will have an OP related fracture in their lifetime • OP is responsible for more than 1.5 million fractures annually .
OP by the Numbers Continued • 2 million American men have OP, 80,000 men suffer a hip fracture an up to one third of these men die within one year • Estimated national direct expenditures (hospital and nursing homes) for OP related fractures $13.8 billion annually
Osteoporosis: Definition • A chronic, progressive condition associated with deterioration of bone tissue that results in low bone mass. As the condition progresses bone fragility increases leading to increased risk of fracture. • Osteopenia is bone that is not as dense as normal bone and is a precursor to osteoporosis.
Osteoporosis: Importance • OP is a major health concern for 2 reasons. • Osteoporotic fractures, most commonly of the vertebrae, femur, and wrist are associated with increased morbidity and mortality. • As the fraction of elderly individuals in the population increases, OP will become more prevalent.
Osteoporosis: Prevalence • Based on Bone Mineral Density data • 6 to 7 million non-institutionalized older U.S. women have osteoporosis • 12-17 million additional women have osteopenia which also increases risk of fracture
Osteoporosis: Diagnosis • Suspected by presence of risk factors. • Bone Mineral Density determination. • Like hypertension and atherosclerosis, osteoporosis can be defined by an intermediate outcome—in this case, low bone mineral density or BMD.
Nonmodifiable * Personal history of fracture as an adult * History of fracture in first degree relative. Caucasian race Advanced Age Female sex Dementia Poor Health/frailty Potentially Modifiable * Smoking * Low Body Weight (<127 lbs) Estrogen deficiency: Early Menopause (<45 yr) or Prolonged amenorrhea Excess alcohol intake Sedentary lifestyle Low calcium intake Inadequate physical activity Poor health, poor eyesight and recurrent falls. Risk Factors in Osteoporosis
Bone Mineral Density Determination in Osteoporosis • Dual X-Ray absorption (DEXA) is most widely used due to excellent precision and accuracy, low radiation exposure, reasonable cost and length of time required to scan a patient. • Sites most commonly assessed • Lumbar spine • Non-dominant hip
BMD Details • BMD measurement at any anatomical site can predict risk of fracture at a distant site. However the measurement of a given site is most accurate for its own risk of fracture.
“Z score” Compares the BMD measured to the BMD of individuals who are at peak bone mass. Usually at age 35 years Predicts the patient’s risk of fracture Aka “% young adult” “T score” Compares the BMD measured with the BMD or age matched peers Indicates if factors other than age may be affecting the patient’s BMD Aka “% age matched” BMD Details: Two Additional Measures
BMD Assessment: Controls • Both Z-score and T-score are expressed as standard deviations above and below the mean and are controlled for weight, ethnic origin and gender.
Fracture Risk • For each 1 standard deviation below the mean of the Z score the risk of fracture nearly doubles • Scores within one SD considered normal • Scores between 1 SD and 2-2.5 SD below the mean considered osteopenia • Scores more than 2-2.5 SD below the mean are considered osteoporosis
Prevention • To understand strategies for OP prevention a person must first understand the biology of bone acquisition and bone loss • There is a balance between bone deposition by cells called osteoblasts and and bone resorption by cells called osteoclasts
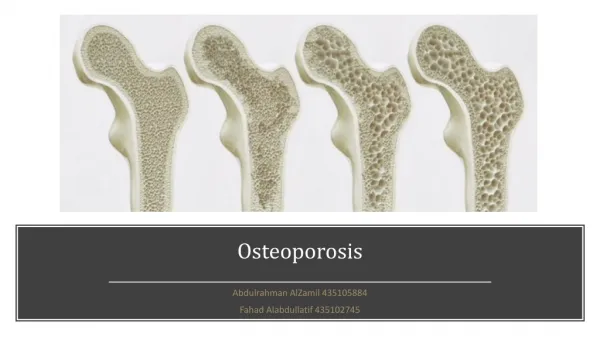
Normal Bone • When resorption and deposition are in balance there is no net change in the amount of bone present
Osteoporotic Bone • After menopause occurs the balance is shifted in favor of increased bone resorption and a loss of bone mass results
Normal Bone Osteoporotic Bone Comparison of Normal and Osteoporotic Bone
Factors in Prevention of Osteoporosis • Nutrition • Level of exercise • Medical conditions • Genetic makeup • Smoking • Alcohol
Nutrition • Calcium is an essential component of many processes in the body and bone serves as a calcium reservoir • Parathyroid hormone maintains calcium in the blood at the expense of bone integrity if dietary calcium is inadequate
Vitamin D • Plays an important role in calcium absorption and bone metabolism • The active metabolite can be synthesized in the skin with the influence of sunlight, but adequate supplementation is a must for individuals who are institutionalized or live in geographic areas where there is inadequate sun exposure
Weight Bearing Exercise: Negative Potential • Exercise in premenopausal women who exercise to a point where menstrual function is lost (exercise induced amenorrhea) a low estrogen state exists and accelerated bone loss can occur as in after menopause • Exercise has potential for trauma for postmenopausal women who have low bone density
Weight Bearing Exercise: Positive Aspects • Weight bearing exercise helps maintain competent bone mass • Sedentary lifestyle contributes to osteoporosis
Medical Conditions • Excess thyroid hormone can cause bone loss • Hyperthyroidism or over medicated hypothyroidism • Steroid therapy can cause bone loss by direct effect on bone, and by suppressing pituitary function and leading to decreased ovarian function and low estrogen states • Rheumatologic, renal, pulmonary and allergic diseases
Smoking • Leads to low BMD • Possible toxic effects on ovary decreasing estrogen levels • Smoking increases rate at which estrogens are cleared from the body
Alcohol Abuse • Those who drink heavily have low bone mineral density compared to nondrinkers and moderate drinkers • Possible direct toxic effect on bone • Heavy drinkers often have nutritional deficiencies
Treatment of Osteoporosis • Hormone replacement therapy • Biphosphonates • Calcitonin • All three treatments work to decrease resorption of bone
Hormone Replacement Therapy • Prevents decrease in BMD • HRT eliminates hot flashes associated with menopause and can also help with other low estrogen related conditions • Most importantly HRT has beneficial effect on cholesterol • May treat some causes of urinary incontinence • May enhance collagen content of skin
HRT Problems • Breast cancer risk? • Uterine stimulation may cause resumption of menses or spotting. Progesterone also required if uterus is present • Breast tenderness • Progesterone alone may help with hot flashes, but recent studies show it does not increase bone mass!!
Evista (Raloxifene HCl) • A new option for prevention of postmenopausal Osteoporosis • Selective Estrogen Receptor Modulator (SERM)
Evista (Raloxifene HCl) • Selective Estrogen Receptor Modulator (SERM) • Binds to estrogen receptor • Estrogen-like effects in some tissue • Estrogen-blocking effects in other tissue
Estrogen Agonist Increases Bone Mineral Density Decreases total cholesterol and LDL cholesterol Estrogen Antagonist Binds to sites in uterus and breast No uterine stimulation No bleeding No uterine cancer risk No need for provera (progesterone) No breast stimulation No breast tenderness Evista: Molecule With Two Active Binding Sites
Evista As an Antiresorptive Agent in Bone • Preserves Bone • Increases BMD (less than estrogens 0.625mg/day) • Normal bone quality • Effects on fracture risk appear encouraging especially for vertebral fractures
Bone Remodeling • After menopause Bone resorption exceeds formation • Evista suppresses resorption • Reduces osteoclast number and activity • Reduces number of resorption sites • As a result reduces bone turnover and improves balance between resorption and formation
Evista: Adverse Events • Hot flashes and leg cramps • Risk of deep vein thrombosis similar to that of traditional HRT, which is quite rare • Contraindicated in patients who: • Are or may become pregnant • History of venous thromboembolic events • Are allergic to Evista
Biophosphonates • Structurally related pyrophosphate which plays an important role in bone metabolism • Fosamax (alendronate) and Didronel (etidronate) are the two most common • BMD increases seen with Fosamax likely the largest compared to all other current treatment options
Biophosphonates: Problems • Didronel if taken daily can lead to bone demineralization so it is dosed every 3 months for 14 days • Stomach upset, esophageal irritation and strict dosing instructions complicate therapy • Not to be used in patients with gastrointestinal disorders
Calcitonin • Available in nasal spray • Has analgesic effect on back pain from osteoporosis • Effective in slowing progression of osteoporosis • Can not be used if individual is allergic to fish products
Combination of Therapies • No current studies available • Literature suggests considering combination therapy when HRT alone fails to stem progression of osteoporosis
Additional Information • www.osteo.org • http://odp.od.nih.gov (NIH)
Osteoporosis Questions?
Topics • If you have any medically related topics you would like presented please let us know.
The End • October 13, 1999