Download
1 / 40
800 likes | 2.33k Views
Cannabinoids. Pharmacology 2008. Cannabinoids. Compounds with pharmacological profile similar to -9-THC (main psychoactive component in marijuana). Research regarding cannabinoids takes place within a controversial sociopolitical climate.

E N D
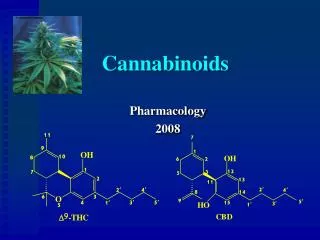
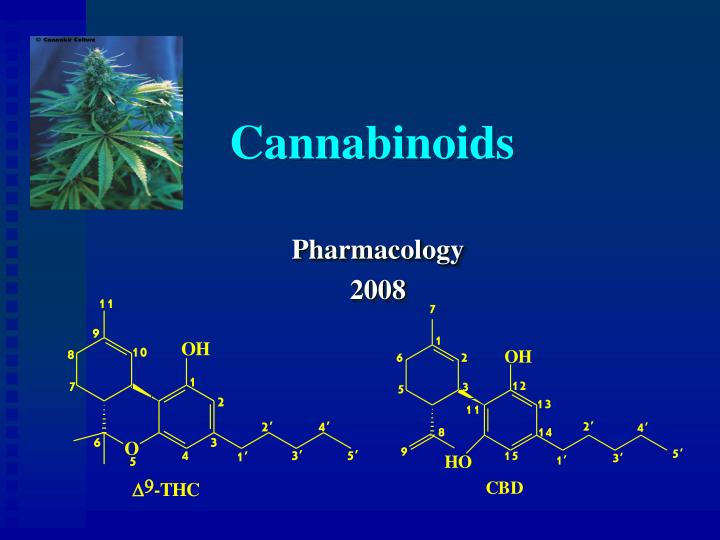
Cannabinoids Pharmacology 2008
Cannabinoids • Compounds with pharmacological profile similar to -9-THC (main psychoactive component in marijuana)
Research regarding cannabinoids takes place within a controversial sociopolitical climate
Cannabis has been used as an analgesic for centuries • Surgical anesthetic in China • Pain of childbirth in ancient Israel • Analgesic throughout Asia through the middle ages
Extracts of cannabis were adopted into British Pharmacopoeia mid 1800s and later the American Pharmacopeia • Widely used as sedative, hypnotic, anti-convulsant • Late 19th and 20th century
With changes in the sociopolitical climate Cannabis was dropped from the British pharmacopoeiain 1932 and the US in 1941 • Clinical use had virtually disappeared in Europe and North America
Contemporary Medicinal Cannabis Use • In many countries eg. Jamaica, India continues to be used • With increasing science supporting analgesic and other therapeutic effects resurgence of interest in the West
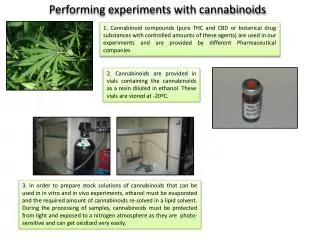
Herbal cannabis • Resins concentrated in glandular trichomes • Function of resin unknown • 3 months from seed to flower
Number of Pubmed citations per 5 year period regarding “cannabinoid” and “cannabis” research
1964 D9-THC synthesized and structure identified (Gaoni & Mechoulam) 1980s Synthetic cannabinoids 1988 CB1 receptor identified (Devane et al.) 1990 CB1 receptor cloned (Matsuda et al.) 1992 CB2 receptor (Kaminski et al.) 1992 Anandamide discovered (Devane et al.) 1993 CB2 receptor cloned (Munro et al.) 1995 2-arachidonylglycerol identified (Mechoulam, Sigiura) 1994-7 Receptor antagonists (Rinaldi-Carmona et al.) 1998 Endogenous ligands shown to be analgesic (Walker et al.)) 1998 CB1 receptor “knock out” mice (Ledent et al. , Zimmer al.) 2000 CB2 receptor “knock out” mice (Buckley et al.) 2001 Noladin -ether identified 2001+ Synthetic cannabinoids, more on the endogenous system, biosynthesis and degradation, delivery systems etc. Milestones in Cannabinoid Pharmacology
Principal Cannabinoids Compounds with a skeleton made of a resorcinol type ring with a terpene moiety derivative attached to it (around 70 identified)
Cannabinoid Receptor Agonists • Cannabinoid receptor agonists can be subdivided into four groups according to their chemical structure. They all have pharmacological and behavioural effects similar to delta-9-THC. • Classical cannabinoids – plant-derived cannabinoids e.g. delta-9-THC, CBD • Eicosanoid cannabinoids – animal-derived cannabinoids e.g. anandamide; 2-AG • Non-classical cannabinoids – synthetic cannabinoids e.g. CP55940; HU-210 • Aminoalkylindoles – synthetic cannabinoids e.g. WIN55212
Pharmacological actions of THC • Psychotropic • Initial euphoria and relaxation • Followed by a depressant period • Alterations memory and cognitive perceptual abilities • Immuno-suppressive/ immuno-modulation • Cardiovascular (tachycardia, orthostatic hypotension, peripheral vasodilation) • Analgesic • Anti-emetic • Appetite stimulant
Pharmacological Effects of CBD • Anticonvulsant • Analgesic • Anti-anxiety • Anti-psychotic • Anti-inflammatory • Anti-arthritic • Immunosuppresive
H2N extracellular intracellular G-protein HOOC Human cannabinoid receptors • CB1 receptors • Present mainly in brain and spinal cord • CB2 receptors • Present in spleen and immune cells • both types are 7-helix transmembrane receptors, coupled to G-proteins
Distribution of CB1 Receptors • hippocampus (MEMORY) • basal ganglia, cerebellum (MOVEMENT) • cerebral cortex • nucleus accumbens(REWARD) • PAG midbrain, RVM (rostral ventrolateral medulla), superficial spinal dorsal horn & DRG,peripheral and central terminals of primary afferent neurons(PAIN) • hypothalamus, pituitary • amygdala, • nucleus solitary tract • Unlike the opioids CB1 are sparse in the brainstem
Endogenous Cannabinoid System • Existence of a receptor in the body suggests that there is an “endogenous agonist” or marijuana like chemical that is naturally produced and acts at the receptor • First two endocannabinoids discovered • Anandamide (1992) • 2-arachidonylglycerol (1995)
Endogenous Ligands O OH C O OH 2-arachidonoyl glycerol
Tissue damage Phospholipids Biosynthesis of endocannabinoids and the arachidonic acid pathway Phospholipase A2 Phospholipase C Arachidonic acid Anandamide 2-AG Noladin NADA Virodhamine Lipo-oxygenase COX1 & COX 2 Leukotrienes Prostaglandins Thromboxane Prostaglandins Prostacyclins
Agonists Pain Anti-emesis Appetite stimulation Anti-spasticity Neuro-protection Intra-ocular pressure in glaucoma Anti-inflammatory Tumor suppression Anti-oxidant activity Immune modulation Sexual dysfunction Psychiatric applications Vascular modulatory Antagonists Addiction control Anorexiants in obesity Potential Therapeutic Applications of Cannabinoids
Therapeutic Applications Pain as an example
Location of CB1 receptors of importance to pain related transmission
Cannabinoid Sites of Action Supraspinal descending inhibition Spinal Peripheral
CB receptors are linked to inhibitory G protein Inhibit adenylyl cyclase cAMP Opening potassium channels: cell firing Closing voltage dependent calcium channels: release neurotransmitters Overall effect is that of cellular inhibition Similar to opioids Gi/o Signal transduction at the CB receptor (Ameri, 1999)
Editorial, Nature (Wilson & Nicoll, 2001; Ohno-Shosaku et al., 2001; Kreitzer & Regehr, 2001) • Cannabinoids are able to function as retrograde synaptic messengers • Endocannabinoid synthesized and released from postsynaptic neurons • Travels backwards across synapse activating CB1 on the presynaptic axon • Resulting in supression of neurotransmitter release
Peripheral cannabinoid effects • Endocannabinoids are present in skin in concentrations 5-10X that in brain • CB1 and CB2 receptors are located peripherally • Peripheral anti-nociception by topical cannabinoid demonstrated in preclinical models
PainStudies in Awake Behaving Animals • Pre-clinical work has demonstrated that cannabinoids block “pain”/nociceptive responses in every acute pain model tested (Walker, 2001) • Effective against thermal, mechanical and chemical induced pain, comparable to opioids in potency and efficacy • In models of chronic pain cannabinoids exhibit even greater potency and efficacy in models of inflammatory and neuropathic pain
Electrophysiological studies of nociceptive neurons in spine and thalamus • Extracellular single neuron recordings • Responses of the neurons to a variety of noxious stimuli • Found cannabinoids produced profound suppression of cellular nociceptive responses
Effects of Cannabinoids on Nociceptive Neurons Summary • High potency (effects at 75 g/kg IV) • High efficacy (>80% in response to noxious stimuli) • CB1 receptor mediated • Suppression of WDR and nociceptors but not mechanoreceptors • Spinal and thalamic neurons affected similarly • Suppression of behavioral and neurophysiological responses to a variety of noxious stimuli • Behavioral analgesic time course was highly correlated with neuronal suppression of nociceptive evoked activity
Evidence for Endogenous Pain Modulation by Cannabinoids • Administration of cannabinoid antagonists: • leads to dose dependent hyperalgesia • blocks the analgesia that would normally be elicited by electrical stimulation of the PAG • Using microdialysis in the PAG Walker demonstrated release of anandamide: • in response to e-stim of PAG • and in association with analgesia after injection of formalin into hindpaws
Clinical Trials • 15/18 RCTs examining cannabinoids in treatment of pain have demonstrated a significant analgesic effect • Evidence supports CBs exhibit a moderate analgesic effect in neuropathic and cancer pain • Preliminary evidence for action in other pain such as spinal pain and headache • In Canada 4 cannabinoid agents available • MMAR • Sativex • Cesamet • Marinol • Guidelines are cited (Clark, Lynch, Ware et al.)
Cannabinoids as AnalgesicsControlled Trials re Cannabis Extracts • Multi-centre RCT oral cannabis extract UK • Improved pain and mobility in MS at 15 weeks • Improved spasticity ( Ashworth scale) at 12 months but not 15 weeks (Zajicek CAMS, 2003,2005) • RCTs buccal sublingual spray extract THC/CBD • Statistically significant decrease in pain of brachial plexus avulsion but not by full 2 point reduction(N=48) • Decreased pain and improved sleep in neuropathic pain in 64 patients with MS
Controlled Trials Examining Synthetic Cannabinoid Agonists as Analgesics • RCT of CT-3 (potent analog of THC-11-oic acid) • 21 patients with neuropathic pain • Significant reduction in pain as compared to placebo • Minor side effects (Karst et al., 2003, JAMA;290:1757-62) • Topically applied cannabinoid agonist HU210 attenuated capsaicin induced pain and hyperalgesia in 20 healthy volunteers (Rukwied et al., 2003, Pain;102;283-288)
Important LiteraturePre-clinical • Cannabinoids • A growing literature demonstrates that endocannabinoids potently inhibit the proliferation of CA cells in vitro and in vivo by acting at CB1 receptors • Modulation of key cell signaling pathways • Endocannabinoids (Anandamide,2-AG) inhibit dose dependently the growth of human colon carcinoma (from biopsies) and this effect is reversed by CB1 receptor antagonist (SR141716A) • HU-210 potently inhibits colorectal carcinoma cell proliferation • Stimulation of CB1 receptors by Met-F-AEA inhibits growth of rat thyroid cancer cell and metastases in Lewis lung carcinoma in mice
Algorithm for Pharmacotherapy of Chronic Pain full assessment of pain condition including addiction screen topicals moderate to severe pain mild to moderate pain nociceptive neuropathic • start a nonopioid analgesic such as acetaminophen or a NSAID • add codeine if necessary nociceptive and neuropathic sleep disturbance present start an anticonvulsant (eg. gabapentin, pregabalin) or tricyclic(eg. DSI,NTI,AMI) start a broad spectrum analgesic antidepressant (eg. DSI,NTI,AMI) start a continuous release opioid stronger than codeine combination pharmacotherapy, if one agent is inadequate to control pain, two or more agents may be necessary (eg. anticonvulsant, tricyclic and opioid) cannabinoids
Labs around the world are working on: • Identification of compounds that retain therapeutic effects without the side effects • Alternative methods of delivery • Manipulation of the endocannabinoid system • Endocannabinoids are synthesized and degraded by what appear to be relatively selective enzymes • A selective transporter for the re-uptake of anandamide may exist (evidence mixed at present, controversial)
In summary the current literature supports that there is a complete endo-cannabinoid system in the body that regulates various physiological processes in brain and peripheral tissues and and there is significant potential to manipulate this system in treating human,pain,suffering and disease.