Download
1 / 22
270 likes | 1.27k Views
Transtibial Amputation. Sarah Kitchin Erica Patterson. Living Without A Leg. Outline. Statistics on Amputation Transtibial and Transfemoral Differences Fitting Balance Biomechanics Conclusion. Amputation Facts. 1,285,000 People Living with Limb Loss in The U.S. 4.9 per 1,000 people

E N D
Transtibial Amputation Sarah Kitchin Erica Patterson
Outline • Statistics on Amputation • Transtibial and Transfemoral Differences • Fitting • Balance • Biomechanics • Conclusion
Amputation Facts • 1,285,000 People Living with Limb Loss in The U.S. • 4.9 per 1,000 people • Of Those 1,285,000 People: • 39,479 were Transtibial Amputations • 36,478 were Transfermoral Amputations (American Amputee Coalition of America ‘96)
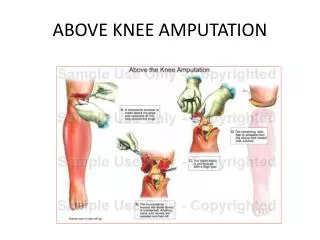
Differences between Transtibial and Transfemoral Amputations • Transfemoral Amputations: • Known as above the knee amputations • Surgeon’s goal is to leave as much residual limb as possible, preserve the adductor muscles, and the remaining soft tissue. (Biomed, ’03)
Differences between Transtibial and Transfemoral Amputations (Cont.) • TranstibialAmputations: • Known as Below The Knee Amputations • The Surgeon’s goal is to leave a cylindrical shaped well-padded residual limb. • Using the gastrocnemius and soleus muscles to create a muscular flap. • Surgery provides some challenges (In Motion, ’03)
Fitting • An exact mold of the residual limb does not make a good socket • Indent in the region around the patellar tendon • Many different types of sockets • Foam of silicone • Hard • Soft (Smith, ’03)
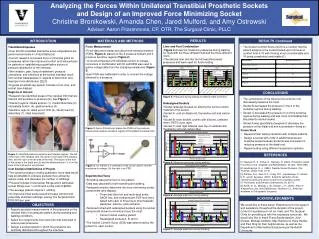
Study on One Type of Socket • 5 Unilateral transtibial amputees • Placed in a pressure chamber • Produces equally distributed pressure at the stump/socket interface • Comfortable and pressure evenly distributed • Still Controversial (Goh, ’03)
Prosthetic Alignment • Alignment is the spatial relationship between the prosthetic socket and foot. • Purpose: • Position the prosthetic socket with respect to the foot so that adverse patterns of force applied to the residual limb are avoided • Produce a normal pattern of gait(Noelle, ’03)
Prosthetic Alignment • (Noelle, ’03)
Prosthetic Alignment Study • Enhance residual limb comfort and maximize walking capabilities in persons with lower extremity amputation • Study suggest prosthetic alignment does promote steady and comfortable walking with a lower extremity prosthesis • Prosthetic misalignment may well lead to instability, discomfort, increased limb loading, and tissue breakdown when applied over a long period of time (Pinzur, ’95).
Balance and Stability Study • Significant differences found between TTA and controls during equilibrium and movement studies. • Transition from bipedal to monopedal • High failure rate for TTA • Same difficulty on sound and prosthetic limb (Viton 00’) • Utilize remaining muscles • Work on speed of contraction, not maximal force of contraction (Gailey 03’)
Walking With a Prosthetic • Prosthetic Walking
Biomechanics - Absorption Phase • Reduction in ground reaction force • Significant difference in knee angles found at heel strike. (Isakov 00’) • Prosthetic absorbs and generates less energy which results in • A more passive limb • Absorption by soft tissue in socket • Presence of isometric contraction by muscles • So as foot strikes, a backward force is instantly created by prosthetic-side hip muscles. (Gailey 02’)
Biomechanics - Deceleration Phase • Hip abductors and adductors and knee extensors muscles are main source of absorption. (Sadeghi 01’) • Fewer gait problems are involved in the swing phase than with the stance. (Walter 04’)
Biomechanics - Acceleration Phase • Hip extensor effort is main compensation of propulsion reduction. (Pailler 04’) • Amputation of ankle reduces the ability of power to be produced through plantar flexion. (Sadeghi 01’)
Biomechanics Summary • Longer motions for amputated side • Step length • Step time • Swing time • Shorter motions for amputated side • Stance time • Single support time (Isakov 00’)
Energy Cost Studies • Energy cost depends on • Gait speed • Efficiency • Not on displacement of center of mass (Detrembleur 05’) • Energy consumption • For transfemoral amputees is more significant than that of transtibial amputees. • Is affected by prosthetic alignment • Is not affected by the use of different prosthetic feet (Schmalz 02’)
Energy Expenditure for Amputation (Janos 05’)
Summary • Transtibial amputations are more common then transfemoral amputations. • There is not one best type of socket fitting • Balance and stability has same difficulty whether on sound or prosthetic limb • Biomechanics are compensated by use of muscles and the combination of longer and shorter motions using amputated side. • Energy costs depend on gait speed and efficiency, not displacement of center of mass
References • Amputation and Limb Deficiency. <http://biomed.edu/Courses/BI108/BI108_2003_Groups/Athletic_Prosthetics/Bkgd>. 14 November 2005. • Amputee Coalition of America. <http://www.amputee-coalition.org/index.html>. 28 November 2005. • Goh, J.C.H., Lee, P.V.S, Chong, S.Y. “Stump/Socket Pressure Profiles cast prosethetic socket.” Clinical Biomechanics. 18 (2003): 237-244. • Detrembleur, Christine. “Relationship Between Energy Cost, Gait Speed, Vertical Displacement of Centre of Body Mass and Efficiency of Pendulum-Like Mechanism in Unilateral Amputee Gait.” Gait & Posture. 21 (2005): 333-340. • Gailey, Robert. “The Biomechanics of Amputee Running.” The O&P Edge. www.oandp.com/edge October 2002. • Gailey, Robert. “Stability Within the Socket Creates Stable World.” The O&P Edge. www.oandp.com/edge September 2003. • Information about Transtibial Prosthetics. <http://www.nupoc.northwester.edu/prosBK.shtml>. 28 November 2005. • Isakov, E. “Trans-tibial Amputee Gait: Time-distance Parameters and EMG Activity.” Prosthetics and Orthotics International. 24 (2000): 216-220. • Janos, Ertl P. “Amputations of the Lower Extremity.” eMedicine http://www.emedicine.com/orthoped January 2005. • Miller, William C. “Balance Confidence Among People With Lower-Limb Amputations.” Journal of the American Physical Therapy Association. (2002).
References (Cont.) • Nadollek, Heidi. “Outcomes After Trans-Tibial Amputation: The Relationship Between Quiet Stance Ability, Strength of Hip Abductor Muscles and Gait.” Physiotherapy Research International. 7 (2002): 203-214. • Noelle, Lannon. “Trans-tibial Alignment: Normal Bench Alignment.” Ortholetter: International society for Prosthetics and Orthotics. <http://home.ica.net/~cocinc/Alignment.html>. July 2003. • Nolan, L. “The Functional Demands On the Intact Limb During Walking for Active Trans-Femoral and Trans-Tibial Amputees.” Prosthetics and Orthotics International. 24 (2000): 117-125. • Pailler, D. “Evolution in Prostheses for Sprinters With Lower-Limb Amputation.” Annales de Readaptation et de Medecine Physique. 47 (2004): 374-381. • Pinzur, Michael S., Cox, William. “The Effect of Prosthetic Alignment on Relative Loading in Person With Trans-tibial Amputation: A Preliminary Report.” Journal of Rehabilitation Research & Development. 32 (1995): 373-378. • Sadeghi, H. “Muscle Power Compensatory Mechanisms In Below-Knee Amputee Gait.” American Journal of Physical Medicine & Rehabilitation. 80 (2001): 25-32. • Shmalz, Thomas. “Energy Expenditure and Biomechanical Characteristics of Lower Limb Amputee Gait: The Influence of Prosthetic Alignment and Different Prosthetic Components.” Gait & Posture. 16 (2002): 255-263. • Smith, Douglas G. M.D. “Transtibial Amputations: Successes and Challenges.” Notes from the Medical Director. • Viton, J M. “Equilibrium and Movement Control Strategies in Trans-Tibial Amputees.” Prosthetics and Orthotics International. 24 (2000): 108-116. • Walter, Ellis. “Gait Analysis After Amputation.” eMedicine.http://www.emedicine.com/orthoped April 2004.