Download
1 / 88
880 likes | 1.27k Views
Ion Channels in the Cardiovascular System in Health and Disease. William A. Coetzee wac3@nyu.edu Tel: 263-8518. Hearts are Composed of Cells. The Cardiac Myocyte. Cells Have Membranes. Channels. Pore. Filter. Gate. Patch Clamping. open. closed. Ion Channels - Gating.

E N D
Ion Channels in the Cardiovascular System in Health and Disease William A. Coetzee wac3@nyu.edu Tel: 263-8518
Channels Pore Filter Gate
open closed
Ion Channels - Gating • A seminal contribution of Hodgkin and Huxley (circa 1940): channels transit among various conformational states • Activation: process of channel opening during depolarization • Inactivation: channels shut during maintained depolarization
+ + Inward Currents Outward Currents Na+ K+ Ca2+ K+ Na+ Ca2+ Cl- Cl- Cl-
Ion Channels • Na+ channels • Ca2+ channels • K+ channels • Exchangers • Pumps
Na+ Channels - Electrophysiology • Rapidly activating and inactivating • A heart cell typically expresses more than 100,000 Na+ channels • Responsible for the rapid upstroke of the cardiac action potential, and for rapid impulse conduction through cardiac tissue
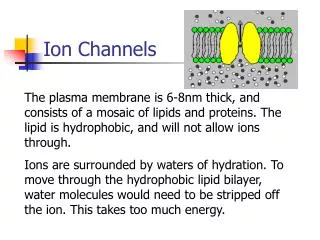
+ Ion Channels – The Traditional View of the Biophysicist out in Ions move through “holes” in the membrane as a result of the electro-chemical driving force (flow of electrical current) The “holes” are selective in that only certain ions are allowed to pass (i.e. Na+ or K+ or Ca2+, etc) The “holes” or “channels” open and close randomly, but open kinetics are influenced by a) voltage and b) time
Ion Channels are Transmembrane Proteins • The first molecular components of channels were identified only about a decade ago by molecular cloning methods • The availability of channel cDNAs has allowed enormous progress in the understanding of the structure and molecular mechanisms of function of ion channels • In addition to the pore forming or principal subunits (often called a subunits), which determine the infrastructure of the channel, many channels (K+, Na+ and Ca2+ channels), contain auxiliary proteins that can modify the properties of the channels
Recent Advances • Important new insights into the mechanisms of ionic selectivity, voltage- and calcium-dependent gating, inactivation and blockade of these channels have been obtained • These efforts recently culminated with the crystallization and high resolution structural analysis of a K+ channel
The Na+ Channel a-Subunit Four repeating units. Each domain folds into six transmembrane helices
Na+ Channels - Structure • Consist of various subunits, but only the principal (a) subunit is required for function • Four internally homologous domains (labeled I-IV) • The four domains fold together so as to create a central pore Marban et al, J Physiol (1998), 508.3, pp. 647-657
Na+ Channels:Structural elements of activation • S4 segments serve as the activation sensors • Charged residues in each S4 segment physically traverse the membrane • Where are the activation gates?
Na+ Channels:Structural elements of inactivation • Multiple inactivation processes exist • Fast inactivation is mediated partly by the cytoplasmic linker between domains III and IV • Slow inactivation?
Na+-ChannelsModulation by auxiliary subunits • Two distinct subunits (b1 and b2) • Both contain: • a small carboxy-terminal cytoplasmic domain, • a single membrane-spanning segment, and • a large amino-terminal extracellular domain with several consensus sites for N-linked glycosylation and immunoglobulin-like folds • The b1 subunit is widely expressed in skeletal muscle, heart and neuronal tissue, and is encoded by a single gene (SCN1B)
Na+-Channels: Genetic Disorders • Congenital long-QT syndrome (LQT3) • Mutations in the cardiac Na-channel gene (SCN5A) • Slowed inactivation • Mutations reside at loci consistent with this gating effect Persistent inward current during AP repolarization, prolonging the QT interval and setting the stage for fatal ventricular arrhythmias
Local anaesthetics (class I antiarrhythmic agents) block Na+ channels in a voltage-dependent manner (S6 segment of domain IV) Block is enhanced at depolarized potentials and/or with repetitive pulsing - modulated receptor model Neurotoxins: tetrodotoxin (TTX) interacts with a particular residue in the P region of domain I µ-conotoxins Sea anemone (e.g. anthopleurin A and B, ATX II) and scorpion toxins inhibit Na+ channel inactivation by binding to sites that include the S3-S4 extracellular loop of domain IV Na+ Channels - Pharmacology
Ion Channels • Na+ channels • Ca2+ channels • K+ channels • Exchangers • Pumps
Ca2+ Channels: Electrophysiology • Calcium influx through voltage-dependent calcium channels triggers excitation-contraction coupling and regulates pacemaking activity in the heart. • Multiple Ca2+ currents: • L, N, P, Q, R and T-type
L-type Ca2+ Current High-voltage-activated Slow inactivation (>500ms) Large conductance (25pS) DHP-sensitive Requirement of phosphorylation Essential in triggering Ca2+ release from internal stores T-type Ca2+ Current Low-voltage-activated Low threshold of activation Small conductance (8pS) Slow activation & fast inactivation Slow deactivation!! Blocked by mibefradil and Ni2+ ions Role in pacemaker activity? Two types of Ca2+ Currents in Heart
The a1-subunit is known to contain the ion channel filter and has gating properties The β-subunit is situated intracellularly and is involved in the membrane trafficking of α1-subunits. The γ-subunit is a glycoprotein having four transmembrane segments. The a2-subunit is a highly glycosylated extracellular protein that is attached to the membrane-spanning δ-subunit by means of disulfide bonds. The α2-subunit provides structural support whilst the δ-subunit modulates the voltage-dependent activation and steady-state inactivation of the channel
Skeletal muscle Mutations in CACNL1A3 (a1S L-type skeletal muscle subunit) Hypokalemic periodic paralysis Malignant hyperthermia (mostly associated with RYR2) Neuronal Mutations in CACNL1A4 (a1A P/Q-type skeletal muscle subunit) Familial hemiplegic migraine Episodic ataxia Spinocerebellar ataxia type-6 Ca2+ Channel a-Subunits Genetic Disorders
Skeletal Ca2+ Channel a-Subunits Genetic Disorders Hyperkalemic periodic paralysis Malignant hyperthermia
Ca2+ Channels: Pharmacology • Three main classes of Ca2+ channel blockers: • Phenylalkylamines (verapamil) • Benzothiazipines (diltiazem) • Dihydropyridines (nifedipine) • Bind to separate sites of the a-subunit(common site: TMs 5&6 of repeat II and TM6 of repeat IV) – equivalent region in Na+ channel causes block by local anesthetics
Ion Channels • Na+ channels • Ca2+ channels • K+ channels • Exchangers • Pumps
Functional Diversity of K+ Channels in the Heart • Voltage-activated K+ Channels • Inward rectifiers • “Leak” K+ currents
Voltage-activated K+ + K+ - “Leak” K+ K+ Inward rectifier Voltage-activated K+ Channels Responsible for repolarization of the action potential and refractoriness (consequences for contractility and arrhythmias)
Voltage-activated K+ + K+ - “Leak” K+ K+ Inward rectifier Inward Rectifier K+ Channels Setting the resting potential and automaticity. Also responsible for repolarization of the action potential and refractoriness (consequences for contractility and arrhythmias)
Voltage-activated K+ + K+ - “Leak” K+ K+ Inward rectifier Leak K+ Channels “Leak” K+ channels: • Plateau (IKP) K+ channels Controlling action potential duration?
K+ Channels - Structure • Both a (principal) and b (auxiliary) subunits exist • Fortuitous correlation exists between the classification system based on function and that based on structure
K+ Channel Principal Subunits Voltage-gated K+ channels Ca2+-activated K+ channels “Leak” K+ channels Inward Rectifier K+ channels 6 TMD 4 TMD 2 TMD Coetzee, 2001
K+ Channel Principal and Auxiliary Subunits Voltage-gated K+ channels Ca2+-activated K+ channels “Leak” K+ channels Inward Rectifier K+ channels 6 TMD 4 TMD 2 TMD KCR1 minK MiRPs KCNK1 KCNK9 KCNK2 KCNK10 KCNK3 KCNK12 KCNK4 KCNK13 KCNK5 KCNK15 KCNK6 KCNK16 KCNK7 KCNK17 SUR Kvb KChAP KChIPs NCS1 Kir eag KCNQ SK slo Kv Kir1 Kir2 Kir3 Kir4 Kir5 Kir6 Kir7 eag erg elk Kv1 Kv2 Kv3 Kv4 Kv5 Kv6 Kv8 Kv9 Coetzee, 2001
Voltage-activated K+ Channels • Transient outward current (Ito) • Slowly activating delayed rectifier (IKs) • Rapidly activating delayed rectifier (IKr) • Ultra-rapidly activating delayed rectifier (IKur) Responsible for repolarization of the action potential and refractoriness (consequences for contractility and arrhythmias)
Transient Outward K+ Channels • Rapidly activating, slow inactivation • Responsible for early repolarization (Purkinje fibers) • Also contributes to late repolarization
Cations TEA, Cs+, 4-AP Class I Disopyramide Quinidine Flecainide Propafenone Class III Tedisamil Other Caffeine, Ryanodine Bepridil D-600 Nifedipine Imipramine Compounds Blocking Ito
Delayed Rectifier Currents IKr and IKs
Delayed Rectifier Current Control Ca-free + Cd Matsuura et al, 1987
Two Types of Delayed Rectifiers 550 ms E-4031 100 pA Sanguinetti & Jurkiewicz, 1991