Download

1 / 18
0 likes | 6 Views
How to Gain Space For General Practitioners

E N D
1 How to gain space How to gain space For For General practitioners General practitioners Prepared by Prepared by Dr. Mohammed Alruby Dr. Mohammed Alruby How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
2 The correction of many malocclusions requires space in order to move teeth into more ideal locations. Space required for correction of: crowding, retraction of proclined teeth, leveling of steep curve of spee, derotation of anterior teeth and for correction of unstable molar relation, the orthodontist is often faced with the dilemma of how to obtain space for these corrections. Planning space is an important aspect of treatment planning. Methods for gaining space: 1-Proximal stripping. 2-Expansion. 3-Extraction. 4-Uprighting of the molars. 5-Derotation of posterior teeth. 6-Proclination of anterior teeth. 7- Distalization. 1-Proximal stripping as a method to gain space: Proximal stripping is a method by which the proximal surfaces of the teeth are sliced in order to reduce the mesio-distal width of the teeth. It also known by the synonyms, re-approximation, slenderization, disking and proximal slicing. Although this procedure is routinely carried out on the lower incisors it can also be done on the upper anterior and buccal segments of upper and lower arches. Indication for proximal stripping: Proximal stripping is usually indicated when the space required is minimal (about 2.5 mm) in these cases, it is possible to avoid extraction of the teeth by performing re-approximation. If the Bolton's analysis shows mild tooth material excess in either of the arches, it is possible to reduce the tooth material by proximal stripping. Contra indication for proximal stripping: Proximal stripping is not carried out in young patients, as they possess large pulp chamber, which increase the risk of pulpal exposure. Patients who are susceptible to caries or those have high caries index. Advantage of proximal stripping: It is possible to avoid extraction in borderline cases where space requirement is minimal. A more favorable over bite and over jet relation can be established by eliminating tooth material excess in either of the arches. More stable results can be established by broadening the contact area thereby eliminating small contact points, which can slip and cause rotation of the teeth. Disadvantage of proximal stripping: The stripping procedure creates roughened proximal surface that attracts plaque. Caries susceptibility is increased as a part of the enamel is removed, leaving behind a roughened area. Patients may experience sensitivity of the teeth. Improper procedure at the hands of the inexperienced operators can result in alteration of morphology of the teeth, creating an unnatural appearance of the teeth. Loss of contact between adjacent teeth may result in food impaction. Diagnostic aids for proximal stripping: Arch perimeter analysis: showing tooth material excess about 2.5 mm over the arch length is a diagnostic criteria favoring re-approximation. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
3 Bolton's analysis: Bolton's analysis revealing an excess of tooth material in either of the arches is an indication to reduce tooth material in that arch. Minimal inter-arch tooth material discrepancies can also be corrected by proximal stripping. Intra- oral periapical radiographs: it is advisable to carefully analyze an accurately taken intra oral radiograph of the region. This would give an idea of the enamel thickness and a rough estimate of the amount of enamel that can be removed from the proximal surface, without exposure of the pulp chamber. Amount of proximal stripping: Not more than 50% of the enamel thickness should be reduced by proximal stripping. Whenever re-approximation is undertaken in a segment of an arch, it is advisable to equally distribute them over all the teeth. Procedure of proximal stripping: Proximal stripping is carried out in one of the following ways: Use of metallic abrasive strips. Safe sided carborundum discs. Long thin tapered fissure burs. Fluoride application: the increased caries susceptibility after stripping is managed by a comprehensive fluoride application program following the procedure. 2-Expansion as a method of gaining space: Expansion is one of the non-invasive methods of gaining space it is usually undertaken in patients having constricted maxillary arch or in patients with unilateral or bilateral cross bite. Expansion can be skeletal or dento-alveolar. Skeletal expansion involves splitting of the mid palatal suture while dento alveolar expansion produces a dental expansion with no skeletal change. Expansion of the palate can be carried out in different ways, which are broadly classified as rapid and slow expansion. Rapid maxillary expansion (RME): Rapid maxillary expansion is splitting of mid-palatal suture and expansion of maxillary arch by application of reciprocal orthopedic force to the teeth and alveolar process on both sides of the arch. RME not only separates the mid palatal suture but also affects the circum-maxillary and circum zygomatic sutural system. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
4 The force level may reach 500 – 700 gm/side. The patient is instructed to turn the jackscrew once /day for 7 to 10 days. After the palate has been widened, a new bone is deposited in the area of expansion, so that, the integrity of the suture is reestablished with 3-6 months. The optimal age for expansion is between 5 to 12 years however some clinician reported palatal splitting at older age, but the results are neither predictable nor stable. Indication of RME: Unilateral or bilateral buccal cross bite with skeletal background. Cleft palate patients with collapsed maxilla. Anteroposterior discrepancy associated with transverse skeletal problems. In case requiring face mask therapy, RME is used along with face mask to loosen the maxillary sutural attachments so as to facilitate protraction. The medical indication for rapid maxillary expansion include nasal stenosis, poor nasal air way. Contraindications: Uncooperative patients. Patients with anterior open bite, steep mandibular plane and convex profile. If RME is done, it should be associated with extra oral intrusive mechanics to counteract the bite opening effect of RME. Single tooth cross bite. Is not carried out after ossification of the mid-palatal suture unless it is accompanied by adjunctive surgical procedures. As the posterior teeth are used as anchors to move the bones parts, the procedure is not indicated in a periodontally weak dentition. Diagnostic aids: The mid palatal suture can be visualized in a maxillary occlusal view radiograph. These radiographs are also useful during treatment to check of mid- palatal split and also to estimate the amount of maxillary expansion achieved. Postro- anterior cephalogram is another valuable diagnostic aid in rapid maxillary expansion procedures to estimate the amount of expansion that has taken place. The effects of RME: Maxillary skeletal effect: The maxillary posterior teeth are used as handles to apply a transverse reciprocal force so as to open the mid-palatal suture. Since the force employed for the procedure is very high, not much of orthodontic changes can be observed. The appliance on activation compresses the periodontal ligament and bends the alveolar process bucally and slowly opens the mid-palatal suture. The opening of the mid-palatal suture is fan-shaped or triangular with maximum opening at the incisor region and gradually diminishing towards the posterior part of the palate. Similar fan shaped or non-parallel opening is also seen in the superior inferior direction. The maximum opening is towards the oral cavity with progressively less opening towards the nasal aspect. The two halves of the maxilla rotate in the sagittal and coronal planes. In the coronal plane the two halves of the maxilla rotate away from each other. The point at which the rotation takes place is around the fronto maxillary suture. In the sagittal plane, the maxilla is found to rotate in a downward and forward direction. Effect on maxillary anterior teeth: the appearance of midline spacing between the two maxillary central incisors is the most reliable clinical evidence of the maxillary separation. The incisor separation is about half of the distance the screw is opened. By three to five months, the midline diastema closes as a result of the trans-septal fiber traction. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
5 Effect on maxillary posterior teeth: the maxillary posterior teeth are used as anchors during rapid maxillary expansion. These teeth show buccal tipping and are also believed to extrude to a limited extent. Effect on alveolar bone: the alveolar bone on the area adjacent to the anchor teeth beds slightly, this due to the resilient nature of the alveolar bone. Effect on the mandible: most authors have observed a downward and backward rotation of the mandible following rapid expansion. This is accompanied by a slight increase in the mandibular plane angle. The reason attributed for the mandibular rotation is the extrusion and buccal tipping of the maxillary molars. Effect on adjacent cranial bones and suture: rapid maxillary expansion not only results in opening of the mid-palatal suture but also has far reaching effects on adjacent cranial structures. In addition, it effects the bones that directly articulating with the maxilla. Effects of RME on the nasal cavity: Increase in the width of the nasal cavity particularly at the floor of the nose adjacent to the mid- palatal suture. The outer walls of the nasal cavity move laterally. Increase in the intra nasal capacity. Increase the alar base width and widening the external naris. As a result of lowering the palatal vault, straightening of the deviated nasal septum may enhanced, which in turn move the septum away from the turbinate bone, thus permit increase in the air volume. Effects of RME on the nasal air way resistance: RME was recommended in patients with bilateral maxillary constriction associated with difficulties in nasal respiration to gain the maximum benefits in the form of buccal expansion together with possible relief of nasal stenosis. Amount of expansion achieved: an increase in maxillary width up to 10 mm can be achieved by rapid palatal expansion. The rate of expansion is about 0.5 mm per day. Types of appliance used: Removable appliance. Fixed appliance: Tooth born: as Isaacson type and Hyrax type. Tissue born and tooth born: Hass expander. Removable appliances: The reliability of these appliances in producing skeletal expansion is highly questionable, although it is possible to split the sutures using removable plates, it nevertheless is unpredictable. Treatment during deciduous and early mixed dentition is considered more favorable in producing appreciable skeletal affects. A removable type of RME device consists of a split acrylic plate with midline screw. The appliance is retained using clasps on the posterior teeth. The disadvantage of a removable rapid expansion appliance is the need for patient co-operation and difficulty in retaining the plate inside the mouth. Fixed appliances: Appliances that are fixed onto the teeth are more reliable and found to produce consistent skeletal effects. Hass type expander: How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
6 The 1st premolar and molar of either side are banded. A thick stainless steel wire of 1.2 mm diameter is soldered on the buccal and lingual aspects connecting the premolar and molar bands. The lingual wire is kept longer so as to extent past the bands both anteriorly and posteriorly. These extensions are bent palatally to get embedded in the palatal acrylic. The split palatal acrylic has a midline screw; the plate does not extend over the rugea area. Isaacson type of expander: This is a tooth born appliance without any acrylic palatal covering; this design makes use of a spring- loaded screw called MINNE expander (developed at the university of Minnesota, dental school). The 1st premolars and molars are banded. Metal flanges are soldered onto the bands on the buccal and lingual sides. The expander consists of a coil spring having a nut that can compress the spring. The coil spring is made to extend between the lingual metal flanges that have been soldered; the expander is activated by closing the nut so that the spring gets compressed. Hyrax type of expander: This type of appliance makes use of special type of screw called HYRAX (hygienic rapid expander) the screws have heavy gauge wire extension that are adapted to follow the palatal contour and are soldered to bands on premolars and molars. Bonded RME: An alternative design of the appliance would be to have a splint covering variable number of teeth on either side to which the jackscrew is attached. Treatment evaluation during RME: Clinically, the most noticeable feature during RME is the appearance of a midline diastema. The amount of the incisors separation is roughly half the amount of jackscrew separation. But the amount of diastema should not be taken as a reliable factor in estimating the amount of expansion. Maxillary occlusal radiograph and PA cephalogram are most reliable in estimating the amount of maxillary expansion. Retention following the RME: Failure to retain the expansion results in relapse. Most authors recommended a retention period not less than 3 -6 months. Isaacson recommended the use of the RME appliance itself for the purpose of retention. Clinical tips for RME: Oral hygiene instruction should be given to the patient and reinforced during the procedure. Orthodontic movement of the anchor teeth should be avoided prior to RME; as mobile teeth do not offer adequate anchorage for palatal split. Maxillary occlusal radiographs should be taken at regular intervals to monitor the expansion. The possible immediate effects of premature appliance removal include dizziness, pressure at the bridge of the nose, pressure under eye, blenching of the soft tissue under the eyes. These symptoms may occur on removal of the appliance for repair and re-cementation; the patients should therefore be kept seated and asked not to stand immediately after appliance removal. Slow expansion: How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
7 The results are more stable when the maxillary arch is expanded slowly at a rate of 0.5 to 1 mm per week. The force generated by such procedures are much lower: 2 to 4 pounds as compared by RME that equal 10 to 20 pounds, unlike in rapid maxillary expansion where the treatment is completed in 1-2 weeks, slow expansion may take as much as 2 -5 months. The slower expansion techniques have also been associated with a more physiologic adjustment to the maxillary expansion, producing greater stability and less relapse potential than the rapid expansion procedures. Appliance used for slow expansion: Jack screw: the various jack screw incorporated in the appliances described for rapid expansion can be used for slow expansion, but with a more spread out activation schedule. The screws used for slow expansion have a smaller pitch than those used in RME. Quad Helix: one of the appliances used to expand a narrow maxilla. The quad helix incorporated four helices that increase the wire length. Therefore, the flexibility and range of action of this appliance is more. The appliance is constructed using 0.038-inch wire and is soldered to bands on the first molars. The quad helix consists of a pair of anterior helices and a pair of posterior helices. The portion of wire between the two anterior helices as called anterior bridge. The wire between the anterior and posterior helices is called palatal bridge. The free wire ends adjacent to the posterior helices are called outer arms. They rest against the lingual surface of the buccal teeth and are soldered into the lingual aspect of the molar bands. The quad helix can be used to expand a narrow arch as well as to bring about rotation of molars. It can be pre-activated by stretching the two molar bands a part prior to cementation. The quad helix is a slow dento-alveolar expansion, but when used it in children during the deciduous and early mixed dentition periods, skeletal mid-palatal splitting can be achieved. Comparison between slow and rapid maxillary expansion Features slow expansion rapid expansion Type of expansion mostly dental skeletal Rate of expansion slow rapid Force used milder greater force Frequency of activation less frequent more frequent Duration of treatment long short type of appliance fixed or removable mostly fixed appliance Age at any age before fusion of bony sutures Retention lesser chance for relapse more chance for relapse N: B: patient who exhibit unusual resistance to separation of the palatine bones may require surgical intervention. This usually occurs in female patients over 16 years of age and male patients over 18 years of age in whom the mid-palatal suture has ossified. Surgical separation may also be required in patients exhibiting increased circum- maxillary rigidity as a result of aging. Maxillary expansion can be brought about by surgery alone or by surgery with a rapid expansion appliance. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
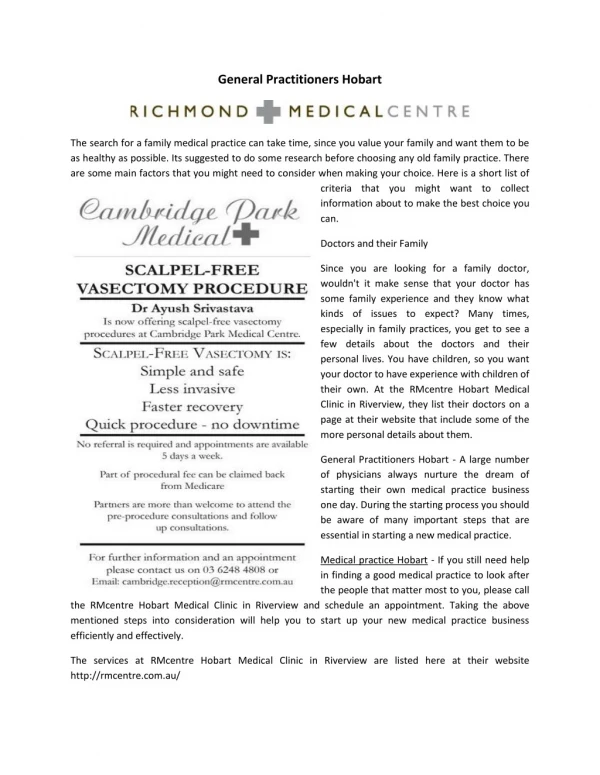
8 The surgical procedures usually carried out are: Palatal osteotomy. Lateral maxillary osteotomy. Anterior maxillary osteotomy. Collapsed arch posterior cross bite Pre- treatment post-treatment RME How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
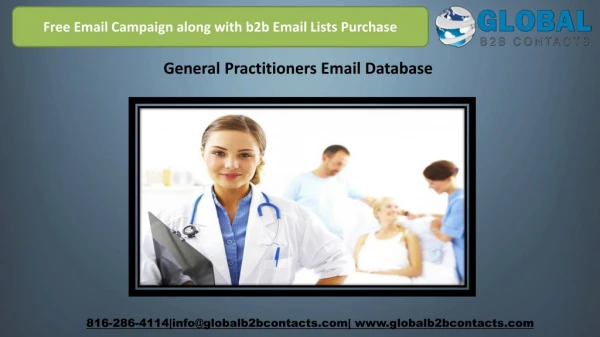
9 Triangular split of maxilla after RME Maxillary slow expansion Mandibular slow expansion 3-Extraction as a method for gaining space The philosophy of extraction in conjunction with orthodontic treatment is not new. Establishment of normal functional occlusion in balance with supporting structures occasionally requires the reduction of one or more teeth. Most extractions are performed as part of a general plane of treatment that also involves the use of appliance. The nature of occlusion and the age of the patient may be important factors in deciding whether or not to resort to extraction. Extraction in orthodontic include serial extraction that carried out as an interceptive procedure during the mixed dentition period and the therapeutic extractions carried out as a treatment procedure for gaining space. Reasons for extraction: It is generally accepted in current orthodontic that if the jaws are not large enough to accommodate the dentition, there is no satisfactory alternative to extraction. If we accept that the jaws cannot be made larger by functional means, the extraction of the teeth in orthodontic treatment will be necessary for the following reasons: How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
10 For relief of crowding: The size of the teeth and the basal bone is too large extent genetically determined; the size of the dental arch is governed mainly by the size of the basal bone and the function of the oral musculatures. If the dentition is too large to fit in the dental arch without irregularity, it is necessary to reduce dentition by extraction of the teeth. It is not usually acceptable to increase the size of the dental arch by expansion because the increase the dental arch dimensions not usually tolerated by the oral musculatures. Criteria of arch length deficiency: Absence of physiologic spacing. Unilateral or bilateral premature loss of deciduous teeth with shift of midline. Malposed or impacted lateral incisors that erupt palatally out of the arch. Marked irregular or crowded upper and lower anterior teeth. Mesial migration of the buccal segment. Lower anterior flaring. Correction of sagittal inter arch relationship: Abnormal sagittal relationship such as Class II or Class III malocclusion may require extraction of such teeth to achieve normal inter arch relationship. The extraction of teeth in such cases helps in establishing normal incisor and molar relationship. Angle's Class II: in most Class II cases, the upper dental arch is forwardly placed so by the extracting in the upper arch it is possible to reduce the abnormal upper proclination. In Class II cases with lower arch crowding or the molar not in full class II occlusion, it may be necessary to extract in both the upper and lower arch to achieve proper inter arch relation and to correct the crowding. Angle's Class III: it is beneficial to avoid extraction in the upper arch because it affects the forward development of the upper arch. Class III cases preferably to extract only the lower arch. Abnormal size and form of the teeth: Teeth that are abnormal in size or form may necessitate their extraction in order to achieve satisfactory occlusion. Such anomalies include macro-dontia; severely hypo plastic teeth, dilacerations and abnormal crown morphology. *** Choice of teeth for extraction: The decision regarding extraction of the teeth is governed by the following: The condition of the teeth: The condition of the teeth must be taken into account in panning extraction, fractured teeth, hypo-plastic tooth, periodontally affected tooth, grossly carious tooth beyond repair are more favorable for extraction than the sound healthy tooth. In assessing the condition of the teeth, the long term prognosis of the teeth is more important than their appearance which should be second consideration. The position of crowding: It is obvious that, if crowding is located in one part of the dental arch it will be more rapid corrected if the extraction is carried out in the same part. Actually the 1st premolars are the most commonly teeth removed to relief the crowding, because they are located in the center of the dental arch and usually near to crowding whether in the anterior or in the posterior segment. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
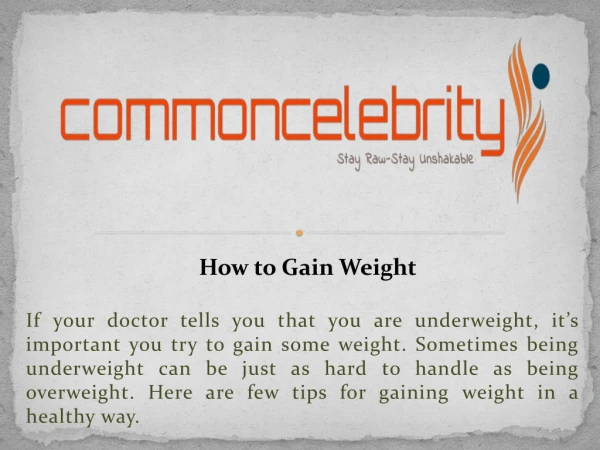
11 The position of the teeth: Teeth which are severely rotated, grossly malposed and would be difficult to align are often the teeth of choice for extraction. Facial profile: Class II: extract, upper 1st premolars and lower 2nd premolars. Class III: extract, upper 2nd premolars and lower 1st premolars. Basal arch dental arch discrepancy. Degree of dento- alveolar prognathism. As a general role the teeth to be extracted should provide the most favorable results with the least amount of tooth movements. Class II extraction case Class I extraction case Consideration of extraction of various individual teeth: 1-Incisor teeth: Should not be extracted unless damaged beyond repair, when the lateral incisors are severely damaged in young children, it may become necessary to remove them and allow the canine to erupt mesially in their spaces then the canine can be reshaped later. In the mandible the space of extracted lower incisors should not be allowed to close by itself because tooth shifting is not predictable. Active closure of the space by an orthodontic appliance is required. Extraction of one of the lower incisors can cause disturbance in the entire occlusion especially in cases with hyperactive mentalis muscle, unpredictable shifting of adjacent teeth, retroclination and flaring of anterior segment and dental arch collapse may be the sequalea. Malocclusion treated by this manner show a tendency to develop an abnormal over-bite and cusp to cusp occlusion in the buccal segment. In rare circumstances, there may be discrepancies in the size of the incisors themselves then consideration may be given to the removal of incisors. The reduction of lower inter canine width often leads to a secondary reduction in the upper inter canine width resulting in upper anterior crowding. Here are some conditions that the lower incisors may have to be extracted: How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
12 If one of the incisors is completely out of the arch with good inter dental contact between the teeth. A lower incisor that was traumatized or exhibiting sever caries, gingival recession, or bone loss may have a poor diagnosis. Presence of sever arch length deficiency is often characterized by the presence of fan shaped flaring out of lower incisor crowns. In these cases it may not be possible to flatten the lower anterior segment by extracting teeth further distally in the arch. So one of the incisors may have to be extracted to improve the crowding and axial inclination of the incisors. In mild Class III cases with lower incisor crowding, one of the lower incisors may be extracted to achieve normal over jet and over bite to relief crowding. In the maxillary arch: the maxillary incisors are rarely extracted as a part of orthodontic treatment; there are some certain conditions that the upper incisors may have to be extracted: An unfavorable impacted incisor that cannot be brought to normal alignment. A grossly carious incisor that cannot be restored. Trauma or irreparable damage of incisors by fracture may indicate their removal. An incisor with dilacerated root that cannot be moved by orthodontic therapy. Occlusions with incisor tooth extraction may shows: A tendency to cusp to cusp relationship on one side of the arch with what called slippage. A tendency for space opening after treatment especially when the basal arch is large. A tendency to increase the over jet. A tendency to develop a deep over bite. 2-Canines: Should not be extracted because of their importance in maintaining facial expression and balance, in certain circumstances, the permanent canine may be removed as in the following cases: Carious beyond repair. Impossible to bring it into normal alignment. When prolonged treatment to be avoided. 3-1st premolars: They are the most common teeth for extraction as a part of orthodontic treatment; the reasons for their extraction are as follows: Their location in the arch is such that the space gained by their extraction can be utilized for correction both in the anterior and posterior region. The contact between the canine and second premolar is satisfactory. -The extraction of the 1st premolars leaves behind a posterior segment that offers adequate anchorage for the retraction of the six anterior teeth. 4-2nd premolars: 2nd premolars may be extracted instead of the 1st premolar in the following cases: When caries beyond repair. When severely malposed, rotated or impacted. In cases of mild space deficiency and the mesial movement of the 1st molars was desired to correct the molar relationship. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
13 If extraction is undertaken in open bite cases, it is preferable to extract the 2nd premolars as their extraction encourage deepening the bite. 1st permanent molars: The first permanent molars may be removed in the following cases: When carious beyond repair. When one 1st molars are removed, the 1st molar on the other side should be removed for symmetrical reasons. ** when one decided to remove the 1st permanent molars due to extensive caries, it is preferable to remove them early before eruption of the 2nd molar because there will be a great chance for 2nd molars to erupt mesially occupying the space. Extraction of the first permanent molars is avoided in the following cases: The extraction of the 1st molar does not give adequate space in the incisor region. The extraction of the first permanent molars will deepen the bite. The second premolars and the second molars may tip into the space. Mastication may be affected. 2nd permanent molars: The extraction of second permanent molars although not common, is advocated for a number of reasons as follow: To prevent third molar impaction, the removal of second molars has been advocated for the prevention of third molar impaction. Upper second molar extraction if carried out prior to the eruption of the third molars, results in satisfactory third molar position. To relieve the impaction of second premolar: the premature loss of second deciduous molars is usually followed by forward drift of the first permanent molars leaving inadequate space for the second bicuspid to erupt. The extraction of second molars in such cases may allow the distal movement of the first permanent molars thereby offering sufficient space for the second premolars to erupt. Lower incisor crowding: very mild crowding in the anterior part of the arch can be relieved by the extraction of the second molars. To enables distalization of the first molars: in cases when the first permanent molars are to be distalized, the extraction of second molars can benefit the procedure. Open bite cases: the extraction of the second molars deepens the bite. Thus they can be considered in open bite cases. Contraindication for extraction of 2nd permanent molars: The third molar is too high in tuberosity or too far in ramus. Delayed eruption or impaction of 3rd molars. Abnormal morphology of the 3rd molar crowns or roots and congenital absence of the third molars. Third permanent molars: 3rd molars may be extracted in one of the following cases: Impacted 3rd molars which interfere with treatment, retention, cause reflex pain or infection. Malformed third molar: which interfere with occlusion should be removed during or after orthodontic treatment. When distalization is indicated, malformed third molar should be removed. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
14 In cases o treated crowding especially in the mandibular arch, 3rd molars may be removed for retention purpose. Contraindication to extraction as a general: When the basal arches are large enough to accommodate all the teeth in normal alignment. Where the functional forces will render the occlusion unstable and bring about relapse. Slight crowding (less than 3mm on each side which can be treated through distalization by extra- oral forces. Early extraction where the growth can change the pattern established by extraction leading to the flat face edentulous appearance. Border line cases in which the correction of molars rotation can provide an adequate space for aligning the teeth. Reasons against early extraction in orthodontic treatment: Growth of the jaws and face can change the pattern achieved by extraction. Relapse may show itself as spacing at the site of extraction due to functional forces and changes in the interdental ligaments. Balancing extraction: Removal of the tooth from one side of the dental arch results in a tendency for the teeth to move towards the extraction space. The teeth distal to the extraction space moves into the space while the teeth mesial to the extraction space can also moves distally into the space. So the midline of the arch may shift to the side of the extraction space. To avoid the unaesthetic shifts of the dental arch, balancing extraction refers to removal of another tooth on the opposite side of the same arch. Compensating extraction: Refers to the extraction of the teeth in the opposite jaw, and carried out to preserve the buccal occlusal relationship. In Class I relation it is usually advisable to extract in both arches to preserve the buccal occlusal relationship. 4-Distalization as a method to gain space: One of the techniques that have gained popularity in recent times is distalization of the molars. Distalization procedures are aimed at moving the molars in distal direction so as to gain space. This approach is becoming popular due to the fact that extraction can be avoided. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
15 Distalization of maxillary molar assumes significant value in the treatment of mild to moderate Class II molar relation associated with normal mandible. Thus by distalizing molars in these cases, extraction of the teeth can be avoided. Distalization can be brought about by the following methods: Extra-oral methods: The most frequently used extra-oral distalizing appliances are the headgears. The headgear assembly consists of: Force delivering unit- face bow- J hook. Force generating unit. Anchorage unit –head cap, neck strap. The basic philosophy of using headgears is to pit the molars against extra-oral anchor units as the occiput or the cervical regions, the forces generated by the force generating units can be adjusted so as to distalize the maxillary molars. Bilateral as well as unilateral distalization is possible using headgears. The forces can be so adjusted that the molars undergo bodily or a distal tipping movement in the posterior direction. A distal tipping movement is only recommended in cases with horizontal growth pattern cases with a square face and deep bites in excess of normal. In such cases, the tipping helps in opening the bite as well as increasing the lower anterior facial height. The treatment using head gears is most effective before the eruption of the second permanent molars. Also the patient compliance is critical for successful results to be achieved. This refers not only regular wear but also the number of hours of wear. A minimum of 12 to 14 hours of wearing is recommended for orthopedic effect and 18 to 20 hours for orthodontic effect (molar distalization). The use of extra-oral forces for distalization has the following disadvantages: 1-Patient cooperation is essential for timely wear of appliance. 2-The appliances are usually not worn continuously. Thus they are intermittent in their action resulting in prolonged treatment time. Intra-oral methods: in order to overcome the drawbacks of extra-oral appliances, various intra- oral appliances to distalize molars were introduced. Intra-oral appliances generate tooth moving forces by mainly three methods: the use of screws, open coil springs, and wire spring incorporated helices. Magnets have been designed for intra-oral use for distalizing, but are not very popular. The intra-oral appliances take anchorage from the palate and anteriorly placed premolars. By pitting more root surface area and / or the rugea region of the palate these appliances are able to minimize the proclination effect of the reciprocal forces generated while distalizing the molars. Here also the efficiency of the appliances is more before the eruption of the second permanent molars. The following are some of the intra-oral devised used: Sagittal appliances: This is a removable appliance with a screw incorporated for the distalization of the 1st permanent molars. The anchorage is gained by the remaining teeth anterior to the 1st permanent molars. Retention clasps are used to hold the appliance in place, the activation of the screw causes the molars to be pushed distally. These appliances did not gain popularity even though they can be used to distalize the maxillary or the mandibular molars primarily because the control achieved is not good as the other appliances. The molars are tipped distally and true bodily movement is not achieved. The removable nature o the appliance also makes it patient dependent. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
16 Distalization using intra-oral magnets: Magnets have been used along with the fixed orthodontic appliances for the purpose of space closure as well as regaining lost space. For the purpose of distalization they are used in repulsion mode with a Nance button for retention. Magnets are not the preferred mode of distalizing molars due to their disadvantages of coast, size and rapid force decay over distance move. Jones Jig: It consists of an open coil spring placed in the buccal aspect, which generates the required forces when it is compressed. Anchorage support is provided with a Nance appliance. It can be used for both unilateral as well as bilateral distalization. It has been shown to distalize molar teeth even after the eruption of the permanent second molars. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
17 5-Uprighting of tilted posterior teeth as a method to gain space: Tilted posterior teeth always occupy more space. Molars tend to tip mesially when the deciduous second molars are lost early or decay on the distal surface and not restored at the appropriate time with the ideal contour. Uprighting of molars can lead to an increase in the arch length about 1.5 mm. fixed appliances are ideally used for this purpose; space regainers or the various screw appliances are also used frequently. 6-Derotation of posterior teeth as a method to gain space: Rotated posterior teeth occupy more space; de-rotation of these teeth can help regain this space. For a similar degree of rotation, the molars occupy more space as compared to premolars; whereas rotated anterior teeth occupy less space. De-rotation can best achieve using a couple forces equal in magnitude but opposite in direction on the lingual and buccal surfaces of the tooth. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby
18 7-Proclination of anterior teeth as a method to gain space: Proclination of anterior teeth can be undertaken in cases where these teeth are retroclined or their proclination will not affect the soft tissue profile of the patient or the stability results. How to Gain Space for G.P How to Gain Space for G.P Dr. Mohammed Alruby Dr. Mohammed Alruby