Download

1 / 17

E N D
1 Torque in Orthodontics Torque in Orthodontics Prepared by Prepared by Dr. Mohammed Alruby Dr. Mohammed Alruby Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
2 Torque when, where, how? Importance of torque Biomechanics in torque Torque expression in slot 0.018 and 0.022 Expression of torque Mode of ligation and torque Types of torque -Passive -Active Factors affect torque Torque with different appliances Torque in base and face Torque prescription in different techniques Class II malocclusion and torque Torque control in different treatment steps Differential torque Torque clearance Intrusion and torque Torque and intra-oral elastics Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
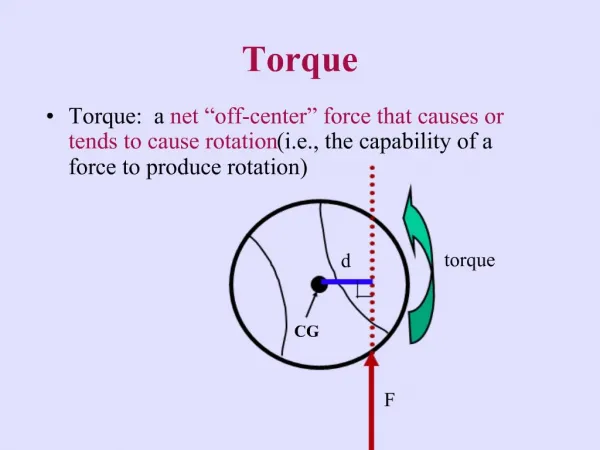
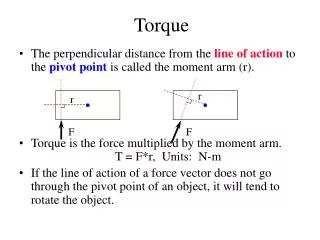
3 as stated by Dr. EARMAN D. RAUCH: Torque is the force that enable the orthodontist to control the axial inclination of the teeth and to place them in the harmonizing positions that are so desirable for a nicely finished results. Torque is the force that gives the operator control over the movement of the roots of the teeth. Torque: movement of root of tooth with little or no movement of the crown in opposite direction by applying couple of force at the same time The center of rotation at incisal edge WHY: -To bring about labiolingual movement of the teeth - To retain the teeth in the cortical bone - To avoid relapse -To give a natural finish to the dentition WHEN: -In third order bends of finishing and artistic positioning in a pre-adjusted edgewise system. - In pre surgical and post-surgical phases for the precise placement for axial inclination of teeth. HOW: Torque in fixed appliance can be employed in different ways 1- By giving a twist in an arch wire -------------– commonly used in edgewise techniques 2-Torque exerted by the bracket itself -------– Pre adjusted edgewise appliance 3- By use of torqueing auxiliary ---------------- widely used in Begg technique. IMPORTANCE OF TORQUE: - Effect on apical bases: One of the objective of orthodontic treatment is reorientation of apical base relationship, maintaining good labial axial inclination of the upper incisors Torque assists the orthodontist in bringing about a desirable change of points A and B, thereafter the desirable facial changes. - Effect on teeth:Proper bucco-lingual inclination of both posterior and anterior teeth is considered important in providing stability and for proper occlusal relationship in orthodontic treatment. - Smile esthetics: Fullness of the smile should be sought through adjustment of the clinical crown torque of the maxillary canines and premolars to their most esthetic appearance in different face types. -Torque and root resorption: Since the first comprehensive study on root resorption by Ketcham, most investigations have confirmed that root resorption is common after orthodontic treatment. In mature young teeth, adult patients and periodontally compromised cases, a thin edgewise arch wire is preferred. The best technical solution to avoid root resorption in light-wire technique would be to apply a light torqueing force that acts interruptedly N: B: M = Fd: With edgewise third order mechanics, rectangular wire engages a rectangular bracket to creates a pair of equal and opposite parallel forces called couple This couple has moment or tendency to rotated (M) and measured as magnitude of force (F) times the distance between the forces (d) Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
4 Proffit: Stated that the simplest way to determine how a tooth will move is by considering the ratio between moment created when force is applied to crown (MF) and counter balancing moment generated by couple within the bracket (Mc) Bio-mechanics in torque: 1-Torque or root movement is achieved by keeping the crowns stationary and applying amount of force acting on the root 2-The center of rotation of tooth is at the incisal edge of tooth movement 3-M / F ratio should be at least 12: 1 to achieve root movement 4-According to Nanda: M / F = 5 / 1 -------- causing uncontrolled tipping M / F = 7 / 1 ------- causes controlled tipping M / F = 10 / 1 ------- causes translation M / F = 12 / 1 ---------causes root torque N: B: When 100gm of force is applied to the tooth (bracket) and center of resistance is 10mm apical to the bracket, will cause a moment of 1000gm. This force alone not cause root movement, to achieve root movement at the level of bracket counter moment of 1200gm is applied through the center of resistance of tooth SO: M / F applied at the bracket is 1200 / 100 = 12: 1 -- , this will cause a distal force of 100gm plus a moment to tip the crown mesially of 300gm –mm By keeping the crown of tooth stationary and applying a counter moment will cause only root movement When M / F ratio applied, tooth appear to rotate around the crown, therefore the center of rotation when the amount to force ratio is 12: 1 is at incisal edge or bracket of crown. N: B: = with no Mc (M / Mf = 0) the tooth rotated around the center of resistance (pure tipping) = as the moment – to – force ration increases (0 > Mc / Mf > 1 ) the center of rotation is displaced further and further away from the center of resistance ----- produce controlled tipping = when (Mc / Mf =1), the center of displacement to infinity and bodily movement (translation) occurs = when (Mc / Mfis less than 1), so the center of rotation is displaced and the root apex will move more than the crown that producing ---- root torque Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
5 Torque expression in 0.018 slot bracket versus 0.022 slot: == 0.018 slot bracket usually has 0.017x0.025 stst wire as working wire which has slop of 6 degree thus, theoretically torque expression in 0.018 slot may be better than 0.022 slot. BUT: 0.018 slot has another shortcoming: 1-Torque prescription for 0.018 tends to be more conservative 2-There is an obvious limitation in a choice of wires and treatment mechanics employed 3-They are not efficient in sliding mechanics as 0.017x0.025 wire does not have sufficient clearance and can be deflected == in 0.022 slot bracket the slop is 10 degree with 0.019x0.025 arch wire must be counteracted by adding 10 -15 degree to the arch wire for utilizing complete built in prescription = in prescription edgewise appliance PEA 0.022 slot is preferred because: 1-During leveling and aligning, these slot have definite advantages in choice of alignment wire 2-0.022 slot are designed for sliding mechanics in which is proven to be more efficient in space closure 3-For fixed functional appliances, orthopedic appliances, or in surgical cases need more stiff wire, full size arch with to avoid deflection SO slot 0.022 is more efficient Expression of torque: = The area of torque application is small and depends on the twist effect of a relatively small size wire, compared with the bulk of tooth SO, the torque is not efficiently expressed by the Preadjusted appliance system, partly due to small area of torque application = In order to slide teeth, it is normal to use 0.019x0.025 stst wire in 0.022 slot because full thickness wire prevent sliding, these wires has slop of about 10 degree depending on the tolerance in bracket and wire manufacturing and amount of wire edge rounding As a result of the relative inefficiency of pre-adjusted bracket in delivering torque, it was necessary to build extra-torque into the incisors, molars, lower premolars bracket in order to meet clinical goal with a minimum of wire bending N: B: Rectangular 0.019x0.025 stst wire in slot 0.022 can yield approximately 10 degree of torque loss. The actual amount depends on variability in both wire and slot but the true torque achieved is less than the value built in slot Mode of ligation: It is difficult to achieve torque control with elastomeric ligation; the use of steel ligation would be effective in maintaining the arch wire in the slot to achieve good torque control Types of torque: A-Passive or harmonizing torque: = Is that torque that incorporated into the rectangular arch wire to accommodate for position of the tubes and or brackets on the buccal and labial surface of the teeth in edgewise system = The buccal surface of bicuspids and molars are usually slopes with height of contour lying more gingivally. This slope produces a degree of angulation of the molars tube and bicuspids brackets So that, the distal portion of the arch wire must torque to fit the brackets and tubes passively Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
6 = on the other hand, if the rectangular arch wire is not torqued, it will forcibly fit the brackets and tubes which induce bucco-lingual tooth movements that alter the bucco-lingual relation of posterior teeth and may create a buccal cross bite. Thus the passive or harmonizing torque is designed to maintain the proper bucco-lingual or labio- lingual relationship of the teeth Harmonizing torque is usually placed in both sides of the arch wire in the distal segment at the inter-proximal space distal to the cuspid, since the buccal slopes of the bicuspids and molars require this torque. How to determine the amount of harmonizing torque? 1-Placing harmonizing torque in the arch wire between cuspid and bicuspid in the right side 2-Place the distal end of the right side of the arch in the right molars tube 3-Observe the relationship of the distal free end of the wire to the left molar tube 4-If the distal free end of the arch wire rest just opposite and on the same horizontal level as the molar tube so, the proper torque is obtained 5-If the distal free end on left side rest gingival to left molar tube so the torque is insufficient 6-If the distal end on left side rest occlusal to the left molar tube so the torque is too much. in the latter two cases, the torque should be adjusted 7-Repeat this procedure for the left side of arch wire 8-When both sides have the proper amount of harmonizing torque, the arch wire can be inserted passively without altering the bucco-lingual relationship of these teeth. BUT now the Preadjusted appliance systems eliminate the needs for such compensatory bends B-Active torque: Torque placed into the rectangular edgewise arch wire either to correct the axial inclination of the teeth or as a part of anchorage preparation ((active buccal root thrust)) Types of active torque: 1-Active labial torque: Torque incorporated in anterior segment of rectangular arch wire to correct the axial inclination of anterior teeth Usually named according to the direction in which the torque will act upon the crown of the tooth: active labial torque will cause the crown to move labially and the root to move palatally. Some investigators named it according to direction of root movement If one wishes to restrict the labial crown movement, then couple of force is required, one force to move the root palatally and the other to prevent labial movement of crown, SO pure movement is obtained This can be achieved by tying back the arch wire to the molars tube and use of class II elastics or headgear to overcome the labial component of torque This type of torque is used during intrusion and retraction of maxillary incisors to avoid flushing of the root against the labial cortical plate which may causes root resorption or fenestration of the labial bone. Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
7 In finishing stages: Selective labial torque should be placed for each tooth to ensure final detailing of the teeth position, for example, 22 degree for 1, 16 degree for 2 and 7 for 3 BUT, the pre-adjusted appliance provides a pre-torqued and pre-angulated brackets that eliminates the needs for such difficult bends. 2-Progressive torque: Torque incorporated into the buccal segment of the arch wire and utilized in the correction of buccal cross bite Starting just distal to the cuspid bracket, a series of bending 15 -20 degree are placed in the arch wire at the interdental spaces between the teeth until 1st molar. The direction of bending is that direction for the desired crown movement as: buccal in maxilla and lingual in mandible The total degree of bending may reach 90 degree at the mesial surface of 2nd molar but when the arch wire is ligated, only 15 – 20 degree is received by each tooth 3-Active root thrust: Active torque placed in the buccal segment of arch wire specially opposite to the mandibular 1st molars to move or thrust the root ag arch wire specially opposite to the mandibular 1st molars to move or thrust the root against the buccal cortex as a form of anchorage re-enforcement Factors affecting torque in orthodontics: 1-Shape of wire: After levelling, rectangular wire is used that express the torque in the roots that tip in all three planes of space 2-Size of wire: Thicker wire has a greater ability to torque, 0.025 ----– than-- 0.022 ------ than-- 0.018 without any twist in wire itself. There is a greater ability of torque in 0.017x 0.025 ------- than-- 0.017x0.022 3-Materials used: Materials with low modulus of elasticity such as Nickel titanium (ni-ti) has reduced torque expression when compared with sst wire {stst wire has 1.5 times torque expression than TMA}, {stst has 2.5 times torque expression than niti} 4-Bracket material: The main fracture strength is much lesser in polycrystalline bracket when compared to monocrystalline ceramic bracket 5-Mode of ligation: The use of steel ligation wire is more successful than elastic ligation because the torque control loss by the loosening of force of elastomeric ligation 6-Bracket height: Bracket height on crown of tooth affect the torque and tip. Poorly positioned bracket will result in imperfectly positioning of teeth and requires a much higher arch wire adaptation 7-Loop design: The torsional stiffness of a looped wire can be distinguished by the two factors are the wire cross section and the loop geometry. Increase in the quantity of wire in the mesiodistal section of the loop and also increasing the diameter of the apex will result in increase of loop ‘s torsional workability Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
8 N: B: The classification of tooth movement associated with edgewise appliance seem to be based upon the type of movements rather than direction. 1- Movement of the First order 2- Movement of the Second order 3- Movement of the third order ----------- We will see here movement of the Third Order Torque with different techniques 1-Torque with removable appliance: Different types of torquing springs can be used which are flexible, easy to construct, easily positioned and adjusted. Bass (1975) has shown that it is possible to perform this movement by pressure in a lingual direction at the gingival margin on the incisors using a double cantilever spring while preventing lingual movement at the incisal edges using a Sved bite-plane 2-Torque with edgewise appliance: = The Edgewise mechanics torques teeth buccally or lingually by placing an activated rectangular wire in a rectangular bracket slot. However, the immediately adjacent teeth receive the equal and opposite reciprocals, which are commonly disregarded. The consequence is a decrease in the facio-lingual discrepancy between adjacent teeth. = Twists in rectangular arch wires seem to be suitable only when reciprocal torque is needed on the adjacent teeth, but one should be aware of high moments emerging in full-sized or nearly full- sized stainless-steel arch wires. = Torque control in finishing stages can be obtained by maintaining a proper moment / force ratio during the time of retraction in extraction cases = To overcome this, torqued slot brackets were introduced by manufacturers in the late 1950s or early 1960s. This design eliminated the need for adding torque to the anterior portion of the upper arch wire 3-Torque with Begg technique: In Begg’s method, the reactions generated by the torquing auxiliaries spread through the arch wire on to the entire arch, rather than pre-dominantly expressing on the adjacent teeth as in edgewise appliance. Originally spurs were bent into the main maxillary arch wire which was made from 0.016-inch arch wire material, to rest against the labial surfaces of the upper central and lateral incisors. The torque force was relayed in a spiral manner along the main arch wire to the anchor molars Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
9 Different types of torquing auxiliary: 1-The four-spur type auxiliary The auxiliary is made from 0.012” Premium Plus wire. However, if only the central incisors require the torque, an auxiliary with two spurs is used 2-Pre-wound torquing auxiliary/ rat-trap type auxiliary, originally devised by Dr Begg in early 1950's. Regardless of the size of wire used in its construction, it is simpler to apply and has the potential to deliver a large force through a greater range of movement than other types of incisor torquing auxiliaries 3-Kitchton’s torquing auxiliary was invented by Dr. John Kitchton, is capable of exerting a great amount of force. It can be made to include central and lateral incisors, or it can be shortened to torque central incisors only 4-For any tooth requiring root torque in the labial or lingual direction, single root-torquing auxiliary proposed by Kesling is a very useful design. It is indicated in case of an upper premolar, which needs buccal root torque to eliminate cuspal interference from its hanging palatal cusp Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
10 5-Reciprocal torquing auxiliary (SPEC design) is used in cases where two adjacent teeth require root torque in opposite directions. The 'Spec' auxiliary could be used for controlling the root movements during the first and second stages if made in lighter 0.009" or 0.010" size wires 6-Franciskus Tan described reverse torqueing auxiliary for controlling the roots of canines or pre-molars design in the 1987. It was reported for the labial root movement of a palatally impacted maxillary canine, whose crown has been aligned but the root is placed palatally and requires labial root torque 7-Mollenhauer's aligning auxiliary (MAA) strives root control from the very beginning, without notably affecting the anchorage and overbite correction, can be used in crowded teeth. This is achieved by using a combination of a stiff base arch wire made from 0.018" Premium plus, and ultra-light root moving forces from the MAA made from the 0.009" supreme grade wire. It can be used after the stage I as the braking mechanism by adding more positive torque into the MAA. In growing brachyfacial cases, labial root torque on the lower incisors can be applied to prevent lingual movement of their root. Whereas, in controlling the mesiodistal root position, a ligature wire is tied to the auxiliary and to the pin to transfer the tipping effect to the tooth 4-Torque prescriptions with edge wise appliance: The Roth prescription: Ronald Roth began to use the straight wire appliance in 1970 when Andrews gave him the first set of high cost prototype brackets that were welded into pinched band material. Since these had inventory problem and Anchorage loss, Roth in 1979 introduced a bracket setup with modified tip, torque, rotations and in out movement of the Andrews standard setup brackets. These second generation of pre-adjusted brackets had more torque in the maxillary incisors which improves esthetics, provides more space for lower anterior teeth, and establishes proper anterior guidance. Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
11 The Vari-simplex discipline: This system was developed and introduced by Dr. R.G. Wick Alexander and is based on edgewise philosophy. Here, ‘Vari’ refers to the variety of bracket types used (Twin, Lewis and Lang) and ‘Simplex’ refers to the principle of KISS (Keep it simple, sir) The Bio-progressive system: This was introduced by Dr. Robert Ricketts and Ruel Bench who combined contemporary edgewise mechanics with solid diagnostic principles and a new approach to sectional mechanics MBT bracket system: = McLaughlin and Bennett worked with Trevisi to re-design the Straight Wire Appliance (SWA) bracket system to complement their treatment philosophy and to overcome the perceived inadequacies of the original SWA. They re-examined Andrews’ original findings and considered additional research input from Japanese sources when designing the third generation of pre- adjusted brackets namely, the MBT system. = Due to the small area of torque application, the pre adjusted appliance system is relatively inefficiency in delivering torque, it is therefore necessary to build in extra torque into the important incisor and molar brackets to achieve the clinical goals with minimum of wire bending [ 5- Torque in lingual technique: Stephen Paige used two separate effective methods such as a torquing auxiliary and torqued ribbon arch for torque control (Figure 11). A torquing auxiliary is similar to the auxiliary in conventional Begg mechanotherapy. The application of force on the tooth is at the incisal edge [28] 6-Torque in self-ligating bracket: = Badawi and coworkers studied the difference in third-order moments that can be delivered by engaging 0.019 x 0.025-in stainless steel arch-wires to 2 active self-ligating brackets and 2 passive self-ligating brackets. = They concluded that as the active clip forces the wire into the bracket slot, the active self-ligating brackets have better torque control. = The amount of arch-wire bracket slop was comparatively less in active self-ligating brackets. The passive self-ligating brackets produced lower moments at low torsion angles and produced higher moments at high torsion that cannot be used clinically. = Compared to passive self-ligating brackets, the active self-ligating brackets have greater clinically applicable range of torque activation, higher expression of torque at clinically usable torsion angles (0°-35°). = Thomali et al evaluated the torque expression in active and passive self-ligating brackets and concluded that there was minor difference in the torque expression of the two brackets. The torque expression increased with increase in engagement angle and also with an increase in slot size Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
12 Torque expression in self-ligating bracket: = active self-ligating bracket seems to have better torque control, direct result of their active clip forcing the wire into the bracket slot = the amount of arch wire bracket slop was considerably less for active self-ligating bracket than passive self-ligating bracket = the active self-ligating bracket expressed higher value than the passive self-ligating brackets at clinically usable torsion angle (0 – 30 degree) Torque in base versus torque in face: = The torque in the base means that the bracket stem is parallel and coincides with the long axis of the bracket slot. But, with the brackets having torque in the face the slot is cut at an angle to the bracket stem, therefore their long axis does not coincide and are not parallel to each other = When the center of the bracket base is placed on FA point the long axis of the bracket stem and bracket slot both are parallel to and are in line with Andrew’s plane. But this is not possible with brackets having torque in the face. Modern bracket systems MBT are developed using computer aided machine the CAD-CAM system. = This allows more flexibility of design, improved bracket strength. The brackets may be finished with all torque in base and torque in face with absolute no difference in slot position Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
13 Torque prescription in different systems a-Andrews Prescription: Lawrence Andrews started the pre-adjusted appliance. In his study he evaluated the occlusion and identified the six keys of occlusion by re-assessing all the previous orthodontic experiences. The third key is described by the torque and was expressed by a bracket containing the angulation, inclination and in-out of each tooth, interrelate with a straight-wire. Andrews prescription Upper inclination Central +7 Lateral +4 Canine -7 1st premolar -7 2nd premolar -7 1st molar -11 b-Roth Prescription: Roth condemn Andrews furnishing of brackets. According to Roth, a large inventory was difficult to handle, so he proposed a new prescription called as the Straight Wire, in which a unique torque value of the upper canines (11°), proposing to use the same brackets for extractions and non- extraction cases. Roth prescription Upper inclination Central 12 Lateral 8 Cuspid 0 1st premolar -7 2nd premolar -7 1st molar -7 c-THE BUTTERFLY SYSTEM: = The butterfly system was introduced by Dr. Jay Bowman and Dr. Aldo Carano. In order to correct the undesired effects produced, in this butterfly system progressive posterior torque was incorporated. = To improve the final buccolingual occlusion, the lower posterior torque is reduced while the upper is increased by flattening the curve of Wilson, reducing inconsistency in posterior overjet, and lowering the bulging of palatal cusps. Butterfly prescription Upper inclination Central 14 Lateral 8 Canine 0 1st premolar -7 2nd premolar -8 Lower Central Lateral Canine 1st premolar 2nd premolar 1st molar inclination -6 -6 -11 -17 -22 -30 Lower Central Lateral Cuspid 1st premolar 2nd premolar 1st molar inclination 0 0 -11 -17 -22 -30 Lower Central Lateral Canine 1st premolar 2nd premolar Inclination -5 -5 -3 -7 -9 Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
14 d-MBT prescription: MBT technique is the third-generation of Straight wire devices. McLaughling, Bennet and Trevisi altered the prescriptions of Roth and Andrews, this alteration is due to the establishment of sliding mechanics, SO that light forces could be used to close the extraction spaces. MBT prescription Upper Inclination Central +17 Lateral +10 Canine 7 / -7 1st premolar -7 2nd premolar -7 1st molar -14 e-ALEXANDER’S THE VARI-SIMPLEX: = An appliance called as the Vari-Simplex Discipline was introducing in the year 1977 by Alexander in which he introduced a system of brackets placed on teeth, employed by orthodontists all over the world and he defines Vari-Simplex Discipline, in which there is specific bracket system utilized in case treatment. = Specific bracket designs are being made for individualized teeth. In this prescription, mainly for non-extraction cases, allows controlled and efficient mandibular arch levelling. Alexander prescription upper inclination Central 14 Lateral 7 Canine -3 1st premolar -7 2nd premolar -7 1st molar -10 f-Self-Ligating Brackets-DAMON System: = The Damon philosophy assert for the lowest frictional resistance of any ligation system with the idea of passive self-ligation technique. = The concept of decreasing the friction allows the force to transfer from the arch wires to the teeth and its supporting structures directly and without any force dissolution by the ligature system. Self-ligating – Damon Upper Inclination Central 12 Lateral 8 Canine 0 1st premolar -7 2nd premolar -7 1st molar -18 Lower Central Lateral Canine 1st premolar 2nd premolar 1st molar inclination -6 -6 6 / -6 -12 -17 -20 lower Central Lateral Canine 1st premolar 2nd premolar 1st molar inclination -5 -5 -7 -11 -17 -22 inclination -1 -1 0 -12 -17 -28 Lower Central Lateral Canine 1st premolar 2nd premolar 1st molar Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
15 Class II malocclusion and torque: Torque of maxillary incisors is critical in establishing an esthetic smile line, proper anterior guidance = Buchin 1957 stated that, reduction of SNA is very desirable in cases with discrepancy in point A and B and is attained by employing strong class II mechanics with anterior lingual root torque or labial crown torque = Bennet and Mclaughin showed, it is necessary to add lingual root torque to upper anterior arch wire and labial root torque to the lower anterior in the arch wire early in space closure and overcorrection in class II rather than attempting to re-establish proper torque that has been lost = high torque brackets were used in the maxillary arch (22degree torque for U12) because the upper incisors more prone to retroclination during retraction = low torque brackets were chosen for the mandibular arch (-6 degree for L12) because negative torque prescription in the lower incisors could counteract the side effect of anterior proclination caused by class II elastics Torque control in different treatment steps: 1-During leveling and alignment: Torque is not expressed only on rectangular stst wire, flexibility of rectangular wires allows early placement and this allows easier torque control than was possible when only steel wire was available 2-During space closure: Loss of torque control during space closure results in upper incisors is too upright at the end of space closure with spaces distal to the canines and consequent unaesthetic appearance == Rapid mesial movement of upper molars can allow the palatal cusp to hang down resulting in functional interferences == rapid movement mesially of lower molar cause rolling of the molars Bite opening curve and torque: Placing bite opening curve in upper arch wire increase the palatal root torque to upper incisors, this beneficial in majority of cases and it is usually unnecessary to add any additional torque bends When the reversed curve is placed in the lower arch result in proclination of lower incisors, this is generally, thus therefore placement of bite opening curve in lower wire approximately 10 -15 degree of labial root torque can be added Deferential torque: When the arch wire with tip back bends is tied into the brackets and tied at the molar tubes different magnitude of moments is produced which are referred as deferential torque Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
16 Torque clearance: Is the amount of play between the bracket and arch wire which depends on the size of arch wire? Arch wire inches stst Amount of play 0.016x0.022 16 – 18 degree 0.017x0.025 13 – 14 degree 0.019x0.025 6 – 8 degree 0.021x0.025 2 – 3 degree Examples: 0.017 x0.025 stst wire in slot 0.022 has approximately 13 – 14 degree play assuming that the wire is completely passive when retraction start WHILE: 0.016 x 0.022 wire has greater amount of tipping and prolonged phase I , II of retraction SO: if the anterior teeth are flared at the beginning, more tipping is required hence a thicker wire will be of limited use, as the effective play will be lesser. If instead the teeth are upright and there is need for more control on the incisors, a thicker wire should be the choice Intrusion and torque control: Utility arch for intrusion creates two-couple force system, the moment of which tend to tip the incisors crown facially and the molar distally. The facial tipping of incisors can be avoided by cinching or tying back the intrusion utility arch, any force that tends to bring the anchor teeth mesially is undesirable. Incorporating twist or torque bend in incisor segment is another way for controlling the tendency of the teeth to tip facially or by using CTA wire which involves no wire bending and needs minimal adjustment, so CTA is better for control of torque. Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby
17 Bi-dimensional techniques: for strong torque control in extraction case: Bi-dimensional slot technique in which pre-torqued 0.018 bracket slot are placed on incisors while 0.022 bracket slot placed on other teeth When wire 0.018 x 0.022 stst wire is engaged, it is fully sized fit into the anterior bracket but leaves clearance 0.004 inch within the buccal bracket SO: in anterior segment can give almost play to the pre-torqued bracket while clearance at buccal segment can facilitate the wire sliding in space closer SO: BDS or BDW technique offer similar capacity for another torque control Torque and intra-oral elastics: 1-Class II elastics: Class II elastics is placed on anterior part of contraction utility arch has an effect of increasing torque during the incisor backward movement Class II elastics pulls downward and backward the anterior loop which raise the anterior segment of the arch and increase the anterior torque progressively with the contraction 2-Class III elastics: Application of class III elastics lead to biomechanics problem to resist the extrusion and lingual tipping elastic force (to avoid gingival dehiscence) Torque in orthodontics Torque in orthodontics Dr. Mohammed Alruby Dr. Mohammed Alruby