Download
1 / 62
680 likes | 1.51k Views
FEVER OF UNKNOWN ORIGIN FUO. Prof. Ferenc Szalay. 1st Department of Medicine of Semmelweis University, Budapest, Hungary. Budapest, 07.11.2005. Fever and Febrile syndromes. TOPICS of the lecture. Thermoregulation Pathogenesis of fever Fever only Fever and Rush

E N D
FEVER OF UNKNOWN ORIGINFUO Prof. Ferenc Szalay 1st Department of Medicine of Semmelweis University, Budapest, Hungary Budapest, 07.11.2005.
Fever and Febrile syndromes TOPICS of the lecture Thermoregulation Pathogenesis of fever Fever only Fever and Rush Fever and Lymphadenopathy
Fever and Febrile syndromes Thermoregulation Pathogenesis of fever Fever only Fever and Rush Fever and Lymphadenopathy Definition Fever of unkown origin (FUO) TOPICS of the lecture
Fever and Febrile syndromes Thermoregulation Pathogenesis of fever Fever only Fever and Rush Fever and Lymphadenopathy Definition Classic New Fever of unkown origin (FUO) TOPICS of the lecture
Fever and Febrile syndromes Thermoregulation Pathogenesis of fever Fever only Fever and Rush Fever and Lymphadenopathy Definition Classic New Causes Fever of unkown origin (FUO) TOPICS of the lecture
Fever and Febrile syndromes Thermoregulation Pathogenesis of fever Fever only Fever and Rush Fever and Lymphadenopathy Definition Classic New Causes Diagnostic strategy Fever of unkown origin (FUO) TOPICS of the lecture
Mechanisms of Heat Regulation To raise Body Temperature To lower Body Temperature
Mechanisms of Heat Regulation To raise Body Temperature Heat generation Obligate heat production Muscular work Shivering
Mechanisms of Heat Regulation To raise Body Temperature Heat generation Obligate heat production Muscular work Shivering Heat conservation Vasoconstruction Heat preference
Mechanisms of Heat Regulation To raise Body Temperature Heat generation Obligate heat production Muscular work Shivering Heat conservation Vasoconstruction Heat preference To lower Body Temperature Heat loss Obligate heat loss Vasodilatation Sweating Cold preference
MAJOR THERMOREGULATORY PATHWAYS I. Skin temperature Core temperature Central thermoreceptors (in hypothalamus, other areas of CNS and abdominal organs) Peripheral thermoreceptors (in skin) Hypothalamic thermoregulatory integrating center
MAJOR THERMOREGULATORY PATHWAYS II. Hypothalamic thermoregulatory integrating center Behavioral adaptations Motor neurons Sympatheticnervous system Sympatheticnervous system Sceletal muscles Skin sweatglands Skin bloodvessels Muscle tone, shivering Skin vasoconstriction, vasodilataion Sweating Control of heat production or loss Control of heat production Control of heat loss Control of heat loss
Fever; Hyperthermia Fever >37.8 °C (100.2°) Elevated body temperature mediated by anincrease in the hypothalamic heat-regulating set point Hyperthermia Increase in body temp. (>41°) that overrides or bypasses the normal homeostatic mechanisms
CAUSES OF FEVER Infection Tissue injury - infarction, trauma Malignancy Drugs Immune-mediated disorders Other inflammatory disorders Endocrine disorders Factitious of self-induced fever
without localizing signs or symptoms Infections presenting as fever Viral Rhinovirus, adenovirus, parainfluenza Enterovirus, ECHO Influenza EBV, CMV Colorado tick fever Bacterial Staphylococcus aureus Listeria monocytogenes Salmonella thyphi, S. parathyphi Streptococci Post animal exposure Coxiella burneti (Q fever) Leptospira interrogans Brucella species Ehrlichia chaffeensis Granulomatous infection Mycobacterium tuberculosis Histoplasma capsulatum
Infections producing Fever and Rush 1. Maculopapular Erythematous Enterovirus EBV, CMV, Toxoplasma gondii HIV Colorado tick fever Salmonella thyphi Leptospira interrogans Measles virus Rubella virus Hepatitis B virus Treponema pallidum Parvovirus B19 Human herpesvirus 6
Infections producing Fever and Rush 2. Vesicular Varicella-zooster Herpes simplex virus Coxackie A virus Vibrio vulnificus Cutaneous petechiae Neisseria gonorrhoea N. meningitidis Rickettsia rickettsii (RMSF) Ehrlichia chaffeensis Echoviruses Viridans-streptococci (endocarditis)
Infections producing Fever and Rush 3. Diffuse erythroderma Group A streptococci (scarlet fever, toxic shock syndr.) Staphylococcus aureus (toxic shock syndr.) Distinctive rush Ecthymia gangrenosum – Pseudomonas aeruginosa Erythema chronicum migrans – Lyme disease Mucous membrane lesions Vesicular pharyngitis – Coxackie A virus Palatal petechiae – rubella, EBV, Scarlet fever Erythema – toxic shock syndr. Oral ulceronodular lesion – Histoplasma capsulatum Koplik’s spots – measles virus
Infections with Fever and Lymphadenomegaly(generalized) ViralMeasles Rubella Hepatitis B Bacterial Scarlet fever Brucellosis Leptospirosis Tuberculosis Syphilis Lyme disease
Infections with Fever and Lymphadenomegaly(regional) Pyogenic infection Sta. aureus, Stre. Tuberculosis Scrofula (tbc. Cervical adenitis) Cat-scratch disease Bartonella Ulceroglandular fever Tularemia Oculoglandular fever Tul., sporotrichosis, etc. Inguinal lymphadenopathy Syphilis, herpes Plague Yersinia pestis
FUO Definition changed 1961 Petersdorf RB et al. 1991 Durack DT et al. More than 200 diseases Major diagnostic challenge
DEFINITION OF FUO Petersdorf RB et al: Fever of unexplained origin: report on 100 cases. Medicine 1961;40:1-30.
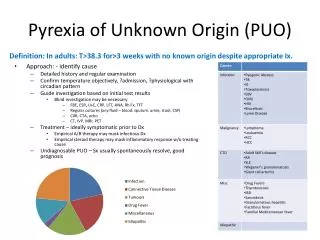
DEFINITION OF FUO 1. Fever ≥ 38.3°C (>101°F) on several occasions Petersdorf RB et al: Fever of unexplained origin: report on 100 cases. Medicine 1961;40:1-30.
DEFINITION OF FUO 1. Fever ≥ 38.3°C (>101°F) on several occasions 2. Duration ≥ 3 weeks Petersdorf RB et al: Fever of unexplained origin: report on 100 cases. Medicine 1961;40:1-30.
DEFINITION OF FUO 1. Fever ≥ 38.3°C (>101°F) on several occasions 2. Duration ≥ 3 weeks 3. Failure to reach a diagnosis despite 1 week appropriate in-hospital investigation or 3 outpatient visits Petersdorf RB et al: Fever of unexplained origin: report on 100 cases. Medicine 1961;40:1-30.
DEFINITIONS Durack DT et al.: FUO- reexamined and redefinied. Curr Clin Top Inf Dis 1991;11:35-51. Knockaert DC et al : FUO in adults: 40 years on. J Intern Med 2003;253:263-275
DEFINITIONS Classical FUO Nosocomial FUO Neutropenic FUO HIV-associated FUO Durack DT et al.: FUO- reexamined and redefinied. Curr Clin Top Inf Dis 1991;11:35-51. Knockaert DC et al : FUO in adults: 40 years on. J Intern Med 2003;253:263-275
NOSOCOMIAL FUO • Hospitalized patient • Fever ≥ 38.3°C(>101°F) on several occasions • Infection not present or incubating on admission • Diagnosis uncertain after 3 days • despite appropriate investigations • (including at least 48-h incubation of microbiological cultures) Examples: Septic thrombophlebitis, sinusitis, Clostridium difficile colitis, drug fever
NEUTROPENIC FUO • Less than 500 neutrophils mm-3 • Fever ≥ 38.3°C(>101°F) on several occasions • Diagnosis uncertain after 3 days • despite appropriate investigations • (including at least 48-h incubation of microbiological cultures) Examples: Perianal infection, aspergillosis, candidemia
HIV-associated FUO • Confirmed HIV infection • Fever ≥ 38.3°C(>101°F) on several occasions • Duration of ≥4 weeks(outpatients) or • ≥4days in hospitalized patient • Diagnosis uncertain after 3 days • despite appropriate investigations • (including at least 48-h incubation of microbiological cultures) Examples:M. avium/M. intracellulare infection, tuberculosis, non-Hodgkin's lymphoma, drug fever
Classification of causative diseases Major disease categories Infections Neoplastic diseases Non-infectious inflammatory diseases (NIID) Minor categories Factitious fever Drug-related fever Habitual hyperthermia (should always be considered before starting FUO work-up)
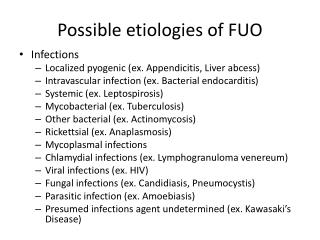
CAUSES OF FUO • INFECTIONSSystemic or Localized
INFECTIONS 1. Systemic infections Most common: Tuberculosis and endocarditis Less common: - Epstein-Barr virus and cytomegalovirus - toxoplasmosis, brucellosis - Q fever, cat-scratch disease, malaria - HIV or opportunistic infections associated with AIDS Tierney LM.(ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
INFECTIONS 2. Localized infections Most common: Occult abscess (liver, spleen, kidney, brain, bone) Less common: - Cholangitis - Osteomyelitis - Urinary tract infection - Paranasal sinusitis LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
CAUSES OF FUO • INFECTIONSSystemic or Localized • NEOPLASTIC DISEASES • Haematological neoplasms • Non-Hodgkin lymphoma • Leukemia • Hodgkin’s disease • Other
CAUSES OF FUO • INFECTIONSSystemic or Localized • NEOPLASTIC DISEASES • Haematological neoplasms Solid tumors • Non-Hodgkin lymphoma Renal carcinoma • Leukemia Colon • Hodgkin’s disease Liver • Other Other
NEOPLASMS Most common: - lymphoma (both Hodgkin's and non-Hodgkin's) - leukemia Less common: - Primary and metastatic tumors of the liver - Renal cell carcinomas - Atrial myxoma - Chronic lymphocytic leukemia - Multiple myeloma LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
CAUSES OF FUO • INFECTIONSSystemic or Localized • NEOPLASTIC DISEASES • Haematological neoplasms Solid tumors • Non-Hodgkin lymphoma Renal carcinoma • Leukemia Colon • Hodgkin’s disease Liver • Other Other • NON-INFECTIOUS INFLAMMATORY DISEASES (NIID) • Collagen diseases, autoimmune dis., vasculitides, Crohn d.
NIID - AUTOIMMUNE DISORDERS Most common: - systemic lupus erythematosus - cryoglobulinemia - polyarteritis nodosa Less common: - Giant cell arteritis - Polymyalgia rheumatica LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
CAUSES OF FUO • INFECTIONSSystemic or Localized • NEOPLASTIC DISEASES • Haematological neoplasms Solid tumors • Non-Hodgkin lymphoma Renal carcinoma • Leukemia Colon • Hodgkin’s disease Liver • Other Other • NON-INFECTIOUS INFLAMMATORY DISEASES (NIID) • Collagen diseases, autoimmune dis., vasculitides, Crohn d. • MISCELLANOUS • Granulomatous, Whipple d.,Cardiac myxoma, Castleman dis.,etc.
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis • Whipple's disease • familial Mediterranean fever • recurrent pulmonary emboli • alcoholic hepatitis • Thyroiditis • Castleman disease • factitious fever LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
MISCELLANEOUS CAUSES • drug-induced fever LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
Agents commonly associated with drug-induced fever Allopurinol Captopril Cimetidine Clofibrate Erythromycin Heparin Hydralazine Hydrochlorothiazide Isoniazid Meperidine Methyldopa Nifedipine Nitrofurantoin Penicillin Phenytoin Procainamide Quinidine AR Roth, and G M. Basello: Approach to the Adult Patient with Fever of Unknown OriginAm Fam Physician. 2003 Dec 1;68(11):2223-8. Review.
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis • Whipple's disease LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis • Whipple's disease • familial Mediterranean fever LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis • Whipple's disease • familial Mediterranean fever • recurrent pulmonary emboli LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005
MISCELLANEOUS CAUSES • drug-induced fever • sarcoidosis • Whipple's disease • familial Mediterranean fever • recurrent pulmonary emboli • alcoholic hepatitis LM. Tierney (ed). Current Medical Diagnosis & Treatment. McGraw-Hill, 2005