Download
1 / 65

E N D
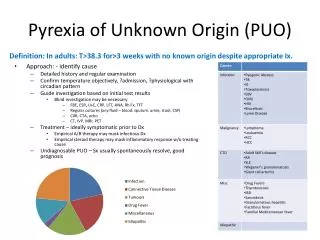
FUO is body temperature ≥ 38.0° C rectally that does not result from transient and self-limited illness, rapidly fatal illness, or disorders with clear-cut localizing symptoms or signs or with abnormalities on common tests such as chest x-ray, urinalysis, or blood cultures.
FUO is classified into 4 categories: • Classic FUO:Fever for > 3 wk with no identified cause after 3 days of hospital evaluation or ≥ 3 outpatient visits • Health care-associated FUO: hospitalized patients receiving acute care and with no infection present or incubating at admission if the diagnosis remains uncertain after 3 days of appropriate evaluation
3. Immune-deficient FUO:Fever in patients with immunodeficiencies if the diagnosis remains uncertain after3 days of appropriate evaluation, including negative cultures after 48 h 4. HIV-related FUO:Fever for > 3 wk in outpatients with confirmed HIV infection or > 3 days in inpatients with confirmed HIV infection if the diagnosis remains uncertain after appropriate evaluation
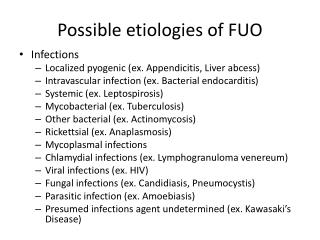
Etiology • Infections (25 to 50%) • Connective tissue disorders (10 to 20%) • Neoplasms (5 to 35%) • Miscellaneous (15 to 25%)
Infections The most common cause of FUO. In patients with HIV infection, opportunistic infections : eg, TB infection by atypical mycobacteria disseminated fungi cytomegalovirus
Connectivetissue disorders SLE RA giant cell arteritis vasculitis juvenile RA of adults (adult Still disease)
The most common neoplasticcauses the incidence of neoplastic causes has been decreasing, probably because they are being detected by ultrasonography and CT, which are now widely used during initial evaluation L lymphoma leukemia renal cell carcinoma hepatocellular carcinoma metastatic carcinomas
Miscellaneouscauses drugreactions deepvenousthrombosis recurrentpulmonaryemboli sarcoidosis inflammatoryboweldisease factitiousfever
SomeCauses of FUO • Cause Abscesses (abdominal, pelvic, dental) • Suggestive Findings Abdominal or pelvic discomfort, usually tenderness Sometimes history of surgery, trauma, diverticulosis, peritonitis, or gynecologic procedure • Diagnostic Approach CT or MRI
Cause Cat-scratchdisease • Suggestive Findings History of being scratched or licked by a cat Regional adenopathy, Parinaudoculoglandular syndrome, headache • Diagnostic Approach Culture (sometimes of lymph node aspirate), antibody titers, PCR te
Cause CMV infection • Suggestive Findings History of bloodtransfusionfromCMV-positive donor Syndromethatresemblesmononucleosis (fatigue, mildhepatitis, splenomegaly, adenopathy), chorioretinitis) • Diagnostic Approach CMV IgM antibody titers Possibly PCR testing
Cause EBV infection • Suggestive Findings Sorethroat, adenopathy, rightupperquadranttenderness, splenomegaly, fatigue Usuallyoccurringinadolescents and youngadults In olderpatients, typicalfindingspossiblyabsent • Diagnostic Approach Serologictesting
Cause HIV infection • Suggestive Findings History of high-risk behaviors (eg, unprotected sex, sharing needles) Weight loss, night sweats, fatigue, adenopathy, opportunistic infections • Diagnostic ApproachTesting for HIV antibodies (ie, ELISA, Western blot) Sometimestesting for HIV RNA (for acute HIV infection)
Cause Infectiveendocarditis • Suggestive Findings Oftenhistory of riskfactors (eg, structuralheartdisease, prostheticheartvalve, periodontaldisease, IV catheter, injectiondruguse) Usually a heartmurmur, sometimesextracardiacmanifestations (eg, splinterhemorrhages, petechiae, Roth spots, Oslernodes, Janewaylesions, joint painoreffusion, splenomegaly)
Diagnostic Approach Serial bloodcultures, echocardiography
Cause Lyme disease • Suggestive Findings Visiting or living in an endemic area Erythemamigrans rash, headache, fatigue, Bell palsy, meningitis, radiculopathy, heart block, joint pain and swelling • Diagnostic Approach Serologictesting
Cause Osteomyelitis • Suggestive Findings Localizedpain, swelling, erythema • Diagnostic Approach X-rays Sometimes MRI (most accurate test), radionuclide scanning with indium-111, bone scanning
Cause TB (pulmonary and disseminated) • Suggestive Findings History of high-risk exposure Cough, weight loss, fatigue Use of immunosuppressants History of HIV infection • Diagnostic Approach Chestx-ray, PPD, interferon-gamma releaseassay Sputumsmear for acid-fastbacilli, nucleicacidamplificationtesting (NAAT), culture of body fluids (eg, gastricaspirates, sputum, CSF)
Cause Sinusitis • Suggestive Findings Prolonged congestion, headache, facial pain • Diagnostic Approach Prolonged congestion, headache, facial pain
Cause Uncommoninfections (eg, brucellosis, malaria, Q fever, toxoplasmosis, trichinosis, typhoidfever) • Suggestive Findings History of travel to endemic areas Exposure to or ingestion of certain animal products • Diagnostic Approach Serologic testing for individual causes Peripheral blood smear for malaria
Connectivetissue • Cause AdultStilldisease • Suggestive Findings Evanescentsalmon-pinkrash, arthralgias, arthritis, myalgias, cervicaladenopathy, sorethroat, cough, chestpain • Diagnostic Approach ANA, RF, serum ferritin concentration, x-rays of affected joints
Cause Giantcell (temporal) arteritis • Suggestive Findings Unilateral headache, visual disturbances Often symptoms of polymyalgiarheumatica, sometimes jaw claudication Tenderness of temporal artery when palpated • Diagnostic Approach ESR, temporalarterybiopsy
Cause Poliarteritisnodosa • Suggestive Findings er, weightloss, myalgias, arthralgias, purpura, hematuria, abdominalpain, testicularpain, angina, livedoreticularis, new-onsethypertension • Diagnostic Approach Biopsy of involved tissues or angiography
Cause Polymyalgiarheumatica • Suggestive Findings History of morning stiffness in shoulders, hips, and neck Malaise, fatigue, anorexia Possibly synovitis, bursitis, pitting edema of extremities • Diagnostic Approach Creatininekinase, ANA, RF, ESR Possibly MRI of extremities
Cause Reactivearthritis • Suggestive Findings Sometimesrecenthistory of infectionwithChlamydia,Salmonella, Yersinia,Campylobacter, orShigella Asymmetricoligoarthritis, urethritis, conjunctivitis, genitalulcerations • Diagnostic Approach ANA, RF, serologictesting for causativepathogens
Cause Rheumatoidarthritis • Suggestive Findings Symmetricperipheralpolyarthritis, prolongedmorningstiffness, subcutaneousrheumatoidnodulesinpressuresites (extensorsurface of ulna, sacrum, back of head, Achilles tendon) • Diagnostic Approach Clinical criteria, ANA, antibodies to double-stranded DNA
Neoplastic • Cause Colon carcinoma • Suggestive Findings Abdominalpain, changeinbowelhabits, hematochezia, weakness, nausea, vomiting, weightloss, fatigue • Diagnostic Approach Colonoscopy, biopsy
Cause Hepatoma • Suggestive Findings History of chronic liver disease, abdominal pain, weight loss, early satiety, palpable mass in right upper quadrant • Diagnostic Approach Abdominal ultrasonography and CT, liver biopsy
Cause Leukemia • Suggestive Findings Sometimeshistory of myelodysplasticdisorder Fatigue, weightloss, bleeding, pallor, petechiae, ecchymoses, anorexia, splenomegaly, bonepain • Diagnostic Approach CBC, bonemarrowexamination
Cause Metastaticcancer Suggestive Findings Symptoms dependent on the site of metastasis (eg, cough and shortness of breath for lung metastasis, headache and dizziness for brain metastasis) Often asymptomatic, discovered during a routine medical evaluation • Diagnostic Approach Biopsy of suspicious mass or node, imaging tests appropriate for area of concern
Cause Myeloproliferativedisorders • Suggestive Findings Frequently asymptomatic, abnormal indices incidentally detected during screening CBC • Diagnostic Approach Testing based on the suspected disorder
Cause Renalcell carcinoma Suggestive Findings Weightloss, nightsweats, flank pain, hematuria, palpable flank mass, hypertension Diagnostic Approach Serum Ca (to check for hypercalcemia), urinalysis, CT of kidneys
Miscellaneous Cause Alcoholiccirrhosis Suggestive Findings Long history of alcohol use Sometimes ascites, jaundice, small or enlarged liver, gynecomastia, Dupuytren contracture, testicular atrophy Diagnostic Approach PT/PTT, alkalinephosphatase, transaminases, albumin, bilirubin Sometimesabdominalultrasonography and CT
Cause Deepvenous thrombosis Suggestive Findings Pain, swelling, sometimes redness of leg Diagnostic Approach Ultrasonography Sometimes D-dimer assay
Cause Drugfever Suggestive Findings Fever coincident with administration of a drug (usually within 7–10 days) Sometimes a rash Diagnostic Approach Withdrawal of drug
Cause Factitiousfever Suggestive Findings Dramatic, atypical presentation, vague and inconsistent details, knowledge of textbook descriptions, compulsive or habitual lying (pseudologiafantastica) Diagnostic Approach Diagnosisof exclusion
Cause Inflammatoryboweldisease Suggestive Findings Abdominalpain, diarrhea (sometimesbloody), weightloss, guaiac-positivestools Sometimesfistulas, perianal and oralulcerations, arthralgias Diagnostic Approach Upper GI endoscopywithsmall-bowelfollow-throughor CT enterography (Crohndisease) Colonoscopy (ulcerative colitis orCrohn colitis)
Evaluation In puzzling cases, such as FUO, assuming that all information was gathered or was gathered accurately by previous clinicians is usually a mistake. Clinicians should be aware of what patients previously reported (to resolve discrepancies) but should not simply copy details of previously recorded history (eg, family history, social history). Initial errors of omission have been perpetuated through many clinicians over many days of hospitalization, causing much unnecessary testing. Even when initial evaluation was thorough, patients often remember new details when questioning is repeated.
Conversely, clinicians should not ignore previous test results and should not repeat tests without considering how likely results are to be different (eg, because the patient's condition has changed, because a disorder develops slowly).
History: History aims to uncover focal symptoms and facts (eg, travel, occupation family history exposure to animal vectors dietary history, that suggest a cause.
History of present illness • duration and pattern (eg, intermittent, constant) of fever. Feverpatterns usually have little or no significance in the diagnosis of FUO, although a fever that occurs every other day (tertian) or every 3rd day (quartan) may suggest malaria in patients with risk factors. • focalpain often indicates the location (although not the cause) of the underlying disorder. Clinicians should ask generally, then specifically, about discomfort in each body part.
Review of systems Includenonspecificsymptoms: weightloss, anorexia, fatigue, nightsweats, headaches. Also, symptomsof connectivetissuedisorders(eg, myalgias, arthralgias, rashes) and GI disorders (eg, diarrhea, steatorrhea, abdominaldiscomfort) should be sought.
Past medical history Shouldinclude disorders known to cause fever: • cancer • TB • connective tissue disorders, • coholiccirrhosis, • inflammatory bowel disease, • rheumaticfever • hyperthyroidism.
Clinicians should note disorders or factors that predispose to infection: • immunocompromise(eg, due to disorders such as HIV infection, cancer, diabetes, or use of immunosuppressants), • structural heart disorders, • urinary tract abnormalities, • operations, and • insertion of devices (eg, IV lines, pacemakers, joint prostheses).
Social history should include questions about risk factors for infection such as : Injection drug use high-risk sexual practices (eg, unprotected sex, multiple partners) infected contacts (eg, with TB) travel possible exposure to animal or insect vectors. Risk factors for cancer, including smoking, alcohol use, and occupational exposure to chemicals, should also be identified.
Family history should include questions about: inherited causes of fever (eg, familial Mediterraneanfever).
Physicalexamination The general appearance, particularly for: cachexia, jaundice pallor noted.
The skin is thoroughly inspected for focal erythema (suggesting a site of infection) and rash (eg, malar rash of SLE); inspection should include the perineum and feet, particularly in diabetics, who are prone to infections in these areas. Clinicians should also check for cutaneous findings of endocarditis, including painful erythematous subcutaneous nodules on the tips of digits (Osler nodes), nontender hemorrhagic maculeson the palms or soles (Janeway lesions), petechiae, and splinter hemorrhages under the nails.