Download
1 / 37
400 likes | 2.38k Views
Neural Tube Defects. Muhammad Syed MD Rajegowda Benamanahalli MD. Neural Tube Defects. Congenital deformities involving the coverings of the nervous system are called neural tube defects (NTDs). . SPINA BIFIDA. ( Latin : "split spine") . Types . spina bifida aperta

E N D
Neural Tube Defects Muhammad Syed MD Rajegowda Benamanahalli MD
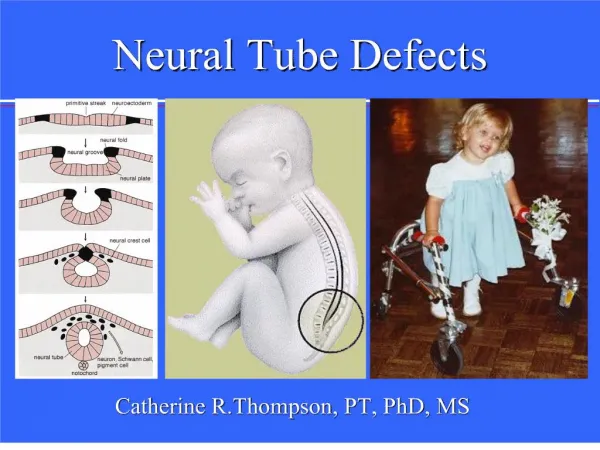
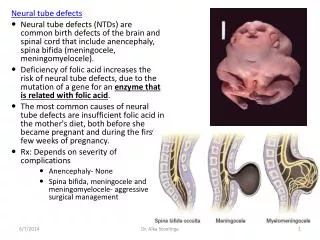
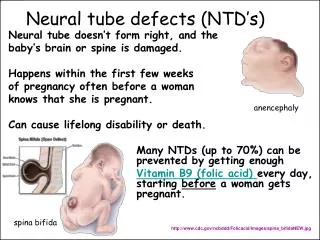
Neural Tube Defects Congenital deformities involving the coverings of the nervous system are called neural tube defects (NTDs).
SPINA BIFIDA • (Latin: "split spine")
Types • spina bifida aperta osseous fusion of one or more vertebral arches is lacking, without involvement of the underlying meninges or neural tissue • spina bifida cystica saclike casing is filled with cerebrospinal fluid (CSF), spinal cord, and nerve roots that have herniated through a defect in the vertebral arches and dura
Spina bifida cystica myelomeningoceles meningoceles Cervical and thoracic regions are the least common sites, and lumbar and lumbosacral regions are the most common sites for these lesions
These lesions are important to differentiate from myelomeningocele because their treatment and prognosis are so different from myelomeningocele. Neonates with a meningocele usually have normal findings upon physical examination and a covered (closed) dural sac. • Neonates with meningocele do not have associated neurologic malformations
In a third, rare type of spina bifida cystica called myelocystocele, the spinal cord has a large terminal cystic dilatation resulting from hydromyelia.
Spina bifida occulta • In this group of neural tube defects, the meninges do not herniate through the bony defect. This lesion is covered by skin (ie, closed), • hairy patch, • dermal sinus tract, • dimple, • hemangioma, • lipoma
Presence of these cutaneous stigmata above the gluteal fold signifies the presence of an occult spinal lesion. Dimples below the gluteal fold signify a benign, nonneurologic finding such as a pilonidal sinus
Signs and symptoms of occult spinal disorders in children include the following: • Radiologic signs • Lamina defects • Hemivertebrae • Scoliosis • Widening of interpedicular distance • Butterfly vertebrae • Cutaneous stigmata • Capillary hemangioma • Caudal appendage • Dermal sinus • Hypertrichosis • Orthopedic findings • Extremity asymmetry • Foot deformities • Neurological problems • Weakness of leg or legs • Leg atrophy or asymmetry • Loss of sensation, painless sores • Hyperreflexia • Unusual back pain • Abnormal gait • Radiculopathy • Urologic problems • Neurogenic bladder • Incontinence
Cranium bifida • midline skull defects • The most benign type of cranium bifidum occultum is the persistent parietal foramina or persistent wide fontanelle. • observation, as these skull defects often close over time.
Encephalocele • anterior neuropore fails to close during days 26-28 of gestation.
Anencephaly • Anencephaly is the most severe form of neural tube defect • Anencephaly the MC major CNS Malformation
defect in notochord development, failure of the cephalic folds to fuse in the midline is failure of the mesoderm to develop; exposing the brain to further insult. brain to be exposed to amniotic fluid, thus destroying the developing forebrain neural cells
Etiology • potato blight, hyperthermia, low economic status, antihistamine and sulfonamide use, nutritional deficiencies, vitamin deficiencies, and anticonvulsant use. carbamazepine, valproic acid,
The reported effects of maternal periconceptional smoking and alcohol consumption on the risk of neural tube defects is of interest. In 2008, results of a population-based, case-control study in California conducted from 1998-2003 were published.Maternal alcohol use increased the risk of neural tube defects, whereas smoking was associated with a lower risk of neural tube defects
Chiari II malformation • Symptoms of a Chiari II malformation can occur anytime after birth and very few patients require decompression after their first year of life for a symptomatic Chiari II malformation. The symptomatic Chiari II presentation can be as subtle as new hoarseness and pneumonia or as obvious as a progressive quadriparesis. A brain and cervical cord MRI in patients with myelomeningocele invariably demonstrates a Chiari II malformation with a herniated vermis and syringomyelia. The surgeon must first and foremost check to see if the ventricular peritoneal (VP) shunt apparatus is functioning. Most of the time, a partial or complete obstruction of a VP shunt (based on a shunt tap or surgical exploration) is the etiology of the new brainstem findings. A shunt malfunction causes the hindbrain to herniate and compress the cord, thus causing many of the presenting symptoms. Timely repair of the shunt leads to a good outcome with reversal of most deficits.
Type I is described as downward herniation of the cerebellar tonsils through the foramen magnum. Type II malformation is herniation of the cerebellar vermis and brainstem below the foramen magnum. Type II malformation also has kinking of the cervicomedullary junction, an upward trajectory of the cervical nerve roots, and associated syringomyelia. The medulla often protrudes below the foramen magnum and into the spinal canal, compressing the cervical cord. The medulla then buckles dorsally and forms a "medullary kink." Also, the fourth ventricle often is below the foramen magnum, and the midbrain tectum forms a sharp corner on midsagittal MRI and looks like a beak. Type II malformations are the subject of this section. Type III malformation is essentially a posterior fossa encephalocele or a cranium bifidum with herniation of the cerebellum through the posterior fossa bone and is a more severe neural tube defect. • The only deviation from the consistent terminology described above is the eponym Chiari type IV malformation. The Chiari type IV malformation consists of cerebellar hypoplasia, not herniation, and is no longer considered a Chiari malformation.
The neonatologist, pediatric geneticist, pediatric neurosurgeon, and pediatric orthopedist should immediately evaluate the child. Possible cardiac abnormalities are evaluated with ultrasonography. Initial ultrasonography of the head may also be performed to evaluate for hydrocephalus. Urologic examination using ultrasonography followed by a complete pediatric urologic evaluation may be performed initially or at a later date. Orthopedic evaluation is performed shortly before discharge because as many as 10% of neonates with a neural tube defect may have hip dislocations
Lipomyelomeningocele this is a skin-covered neural tube defect. The neonate often presents with a skin-covered mass above the buttocks
Questions? • Which of the following is the most common congenital anomaly? A congenital Neural tube defects B congenital Limb defects C congenital heart diseases D congenital Renal agenesis
Which of the following is the most common congenital CNS Malformation ? A Meningocele B Myelomeningocele C Anencephaly D Hydrancephaly