Download
1 / 25
380 likes | 1.46k Views
Lymphatic Filariasis. Dan Imler Morning Report. EPIDEMIOLOGY . W. bancrofti occurs in the following regions: sub-Saharan Africa, Southeast Asia, the Indian subcontinent, many of the Pacific islands, and focal areas in Latin America.

E N D
Lymphatic Filariasis Dan Imler Morning Report
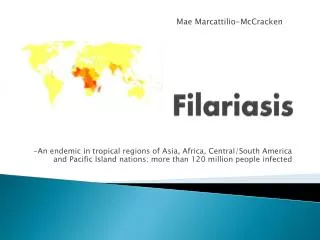
EPIDEMIOLOGY • W. bancrofti occurs in the following regions: sub-Saharan Africa, Southeast Asia, the Indian subcontinent, many of the Pacific islands, and focal areas in Latin America. • B. malayi occurs mainly in China, India, Malaysia, the Philippines, Indonesia, and various Pacific islands. • B. timori is limited to the Timor Island of Indonesia. • Within endemic regions, the infection has a focal distribution that coincides with areas conducive to breeding sites for the mosquito vector.
EPIDEMIOLOGY • It is estimated that more than 120 million people worldwide are infected with one of these three microfilariae. • More than 90 percent of these infections are due to W. bancrofti, and the remainder are mostly due to B. malayi. • Estimates suggest that more than 40 million infected individuals are seriously incapacitated and disfigured by the disease. • A study from India, which accounts for 40 percent of the global prevalence of infection, estimated that a minimum of $842 million is lost each year there, secondary to treatment costs and working days lost from filariasis.
85% of Haiti’s population lives in areas at risk of LF transmission. • According to a 2001 antigen survey, 117 of 133 communes are endemic for LF. • In 2002, an estimated 2,130,000 people (30% of the total population) were thought to be infected. • The parasite responsible for LF in Haiti is Wuchereria bancrofti spread mainly by Culex mosquitoes.
EPIDEMIOLOGY • Adult worms are gradually acquired over years, slowly accumulating and producing microfilariae in infected individuals. • Thus, the prevalence of microfilaremia in endemic communities increases with age. • After the third or fourth decade of life, most people have been exposed and the proportion of infected individuals remains relatively constant.
EPIDEMIOLOGY • New sensitive diagnostic tests reveal that lymphatic filariasis is first acquired in childhood, often with as many as one-third of children asymptomatically infected before age five • The risk of infection in childhood may be related to the maternal immune response during pregnancy. In one study of mother-newborn pairs, there was a 13-fold increased risk of developing childhood Wuchereria infection, compared to uninfected controls, if the mother had active infection and there were absent filarial-specific T cell responses in cord blood at birth. • However, the risk of childhood filariasis was only five-fold higher if there was evidence of T-cell specific immunity in cord blood lymphocytes.
EPIDEMIOLOGY • As with most helminth infections, the adult parasite does not replicate within the human host. Thus, the adult worm burden (as opposed to the microfilarial burden) cannot increase once an individual is no longer exposed to infective larvae, such as after leaving an endemic region. • Since the mosquito vectors are not efficient transmitters of filariasis, a relatively prolonged stay in an endemic area is usually required for the acquisition of infection.
EPIDEMIOLOGY • Unlike most other mosquito-borne infections, several different mosquito species, including Anopheles, Culex, Aedes, and Mansonia species can serve as vectors for transmitting filariasis. • The geographic distribution of these mosquitoes varies, and both urban and rural transmission of disease occurs. • In many tropical and subtropical areas, the prevalence of infection is increasing due to progressive urbanization and increased breeding sites for the mosquito vectors.
LIFE CYCLE • W. bancrofti, B. malayi, and B. timori are all acquired via the bite of mosquitoes. • When mosquitoes bite humans, they deposit third-stage infective larvae into the skin. • These larvae travel through the dermis and enter local lymphatic vessels. Over a period of approximately nine months, these larvae undergo a series of molts and develop into mature adult worms, which range from 20 to 100 mm in length. • These adults reside in the lymphatics, generally several centimeters from lymph nodes. They survive for approximately five years (occasionally up to 12 to 15 years), during which time male and females worms mate and produce microfilariae. • Female parasites can release more than 10,000 microfilariae per day into the bloodstream. These microfilariae are also known as embryonic or first-stage larvae, and measure approximately 200 to 300 µm by 10 µm.
LIFE CYCLE • Mosquitoes, which bite infected individuals, can take up these circulating microfilariae. Within the mosquito, these embryonic larvae develop into second then third stage larvae over a period of 10 to 14 days. The mosquito is then ready to bite and infect a new human host, thereby completing the life cycle. • The interval between acquisition of infective larvae from a mosquito bite and detection of microfilariae in the blood is known as the prepatent period. This interval is usually approximately 12 months in duration.
CLINICAL FEATURES • Most people infected with Brugian or Bancroftian filariasis in endemic areas are asymptomatic, since the development of symptoms relates to the cumulative acquisition of increasing numbers of worms. • Estimates suggest that at most one-third of infected individuals have clinical manifestations. • In endemic communities, clinical symptoms are not usually evident until adolescence or adulthood. The clinical course of lymphatic filariasis includes three distinct phases: asymptomatic microfilaremia, acute episodes of adenolymphangitis (ADL), and chronic disease (irreversible lymphedema), which is often superimposed upon repeated episodes of ADL.
Acute adenolymphangitis • Acute adenolymphangitis (ADL) characteristically presents with the sudden onset of fever and painful lymphadenopathy. • Often there is retrograde lymphangitis, meaning that the inflammation spreads distally away from the lymph node group, which distinguishes it from the pattern typically associated with streptococcal lymphangitis. • ADL is thought to occur because of immune-mediated responses to dying adult worms. It can manifest in a variety of locations, but the inguinal nodes and lower limbs are commonly involved. • The inflammation tends to resolve spontaneously after four to seven days, but recurrences are frequent. • Recurrences are typically seen one to four times per year, but the number of attacks increases with increasing severity of lymphedema. • In addition, secondary bacterial infections can occur related to the breakdown of skin barriers in edematous or elephantatic skin or overlying intensely inflamed lymph nodes.
Filarial fever • Another clinical syndrome is known as filarial fever. This is characterized by acute, self-limiting episodes of fever, often in the absence of any obvious lymphangitis or lymphadenopathy. • Because of the lack of associated features, this syndrome is frequently confused with other causes of fever in the tropics, such as malaria.
Tropical pulmonary eosinophilia • Tropical pulmonary eosinophilia is characterized by nocturnal wheezing. • It is caused by an immune hyperresponsiveness to microfilariae trapped in the lungs and is typically seen in young males.
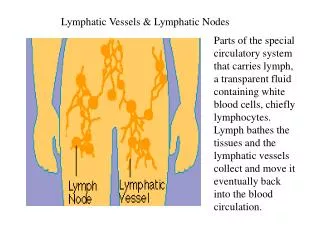
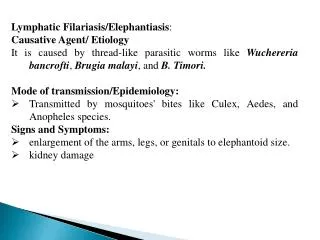
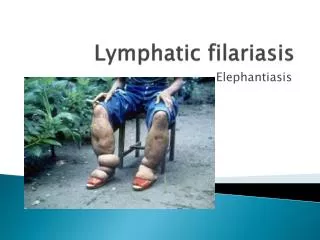
Chronic Lymphedema • Lymphedema, or swelling of a limb related to chronic inflammation of the lymphatic vessels, is a common late sequela of filarial infection. • When the lymph vessels in the inguinal region are involved, swelling of the lower limb(s) ensues. • When axillary lymph nodes are involved, swelling of the upper limb(s) results. • Involvement of the breast can also occur in women. • Pitting edema is present early, but with more chronic inflammation, brawny edema and hardening of the tissues develops, eventually resulting in hyperpigmentation and hyperkeratosis. • When lymphedema is severe, it is often referred to as elephantiasis.
Chronic Lymphedema • The World Health Organization (WHO) has developed a system to grade the severity of lymphedema. • Grade I — Pitting edema that is reversible by elevating the leg • Grade II — Nonpitting edema that does not reverse with elevation of the extremity • Grade III — Severe swelling with sclerosis and skin changes
Chronic Lymphedema • Chronic lymphatic disease can also involve the genitalia, resulting in the development of unilateral or bilateral hydroceles. • Hydroceles can be larger than 30 cm in diameter but are usually painless unless complicated by bacterial infection. • Localization of adult worms in the lymphatics of the spermatic cord can also lead to palpable thickening of the cord. • Lymphatic filariasis of the ovary and mesosalpinx has also been reported.
DIAGNOSIS • Nonspecific test abnormalities – Eosinophilia up to 3000/microL • Blood examination for detection of microfilariae should be performed in all individuals in whom the diagnosis of filariasis is suspected. Bancroftian and Brugian filariasis tend to show nocturnal periodicity. Blood should be drawn between 10 p.m. and 2 a.m. because the greatest number of microfilariae can be found in blood during this peak biting time of the mosquito vectors. The pattern of periodicity can be reversed by changing the patient's sleep-wake cycle. • Antibody tests — Serologic tests for filarial antibodies which detect elevated levels of IgG and IgE are available • Antigen tests — Different methods for detection of antigen in the blood have been attempted using various monoclonal antibodies.
TREATMENT • Diethylcarbamazine — DEC is not distributed for use in the United States but can be obtained from the Centers for Disease Control and Prevention (CDC) under an Investigational New Drug (IND) protocol • Ivermectin — Studies have established that ivermectin given as a single dose in Bancroftian filariasis reduces microfilaremia by approximately 90 percent even one year after treatment • Albendazole — has also been used in filarial infections. Prolonged courses of high dose albendazole have a significant macrofilaricidal effect and result in a gradual decrease in microfilarial levels. • Doxycycline — Initial studies suggested that coxycycline, which has good activity against Wolbachia, leads to sterility of adult worms
Workers in Port-au-Prince clean sea salt before spraying it with a deworming drug and bagging it. The treated salt is then sold at a loss to Haitians. Mass drug administration — This approach reduces both the transmission of infection and disease morbidity. The hypothesis is that once populations have been treated long enough, levels of microfilaremia will remain below that required to sustain transmission. This period has been estimated to be four to six years, corresponding to the usual reproductive lifespan of the adult parasite. Ideally, programs should focus on treating both adults and children.
Uptodate.com • Diagnosis, treatment, and prevention of lymphatic filariasis • Epidemiology, pathogenesis, and clinical features of lymphatic filariasis • NYtimes.com • Beyond Swollen Limbs, a Disease's Hidden Agony • http://www.nytimes.com/2006/04/09/world/americas/09lymph.html