Download
1 / 2
20 likes | 38 Views
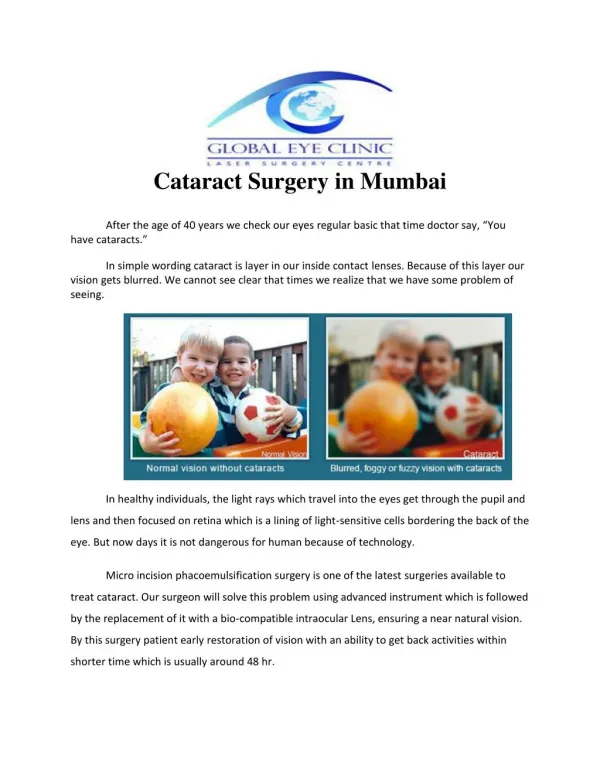
Can you keep using smudgy sunglasses without a single complaint? Having a cataract is something like that. Here's more about the cloudy or sometimes blurry view.<br>

E N D
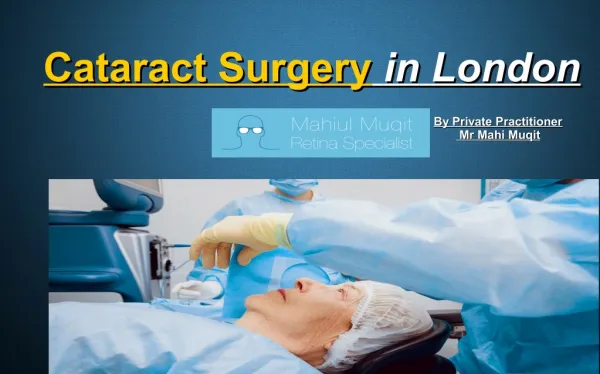
Manual Small Incision Cataract Surgery Having a cataract is a bit like having a dirty windscreen on a car. It can make the view cloudy or foggy or sometimes blurry. It can also cause glare from bright lights, sunshine, and on-coming headlights while driving. When these problems make your normal daily activities difficult, it is time consider the cataract operation. Cataract Surgery has undergone significant changes, beginning with the abandonment of ICCE Intracapsular Cataract Extraction with prescription of thick +10.00D glasses. Kelmen, an American ophthalmologist revolutionized Cataract Surgery in 1967 by introducing phacoemulsification wherein ultrasonic energy is used to emulsify the cataract with placement of IOL intraocular lenses which have now entered a fifth generation mode. The technique of ICCE changed to ECCE (Extracapsular) where the support system of the capsule is left behind to place the IOL. ECCE involved 10mm incision removal of the cataracts nucleus and placement of IOL. However, the large incision had to be closed with sutures and resulted in astigmatism and delayed post-operative period. Phacoemulsification using USG to emulsify the cataracts nucleus brought down the 10mm incisions to 2.2-2.8mm – a key hole option with negligible astigmatism and quick recovery. The problem with Phaco was the cost and its inability to handle rock hard grade 4/5 cataracts without damaging neighboring tissues like the corneal endothelium.
Manual Small Incision Cataract Surgery, MSICS was an innovation by Bluementhal et all in 1992. It was suture less, seamless with few complications and quick post-op recovery without astigmatism. It also required very little equipment and was ‘low cost’ but came with a steep l learning curve. All hard cataracts could now be handled without the fear of damaging neighboring structures as happened with Phacoemulsification. The first such surgery was performed at Aster Hospital, Mankhool on 2nd July 2018, after explaining in detail the procedure to the patient, whose cataract was a grade 5 Brunescence cataract (Cataracta Nigra.) Phacoemulsifucation is not a good option for such cases as the energy used to break these “ROCK HARD” cataracts can damage the corneal endothelium which is the main pump of the cornea which when damaged leads to Corneal blindness. This type of Surgery is not done frequently in Dubai where the patients come early and the cataracts are “SOFT” and easily amenable to phacoemulsification. The patient however kept postponing the surgery as her diabetes was not under control for a long time. Complicating the situation were numerous co morbid conditions directly affecting the Eye Surgery. The team at Aster however controlled and stabilized her clinical condition before we wheeled her to the Operation theater. The post-operative result was excellent with full recovery of vision. The patient feedback was very appreciative of the hospital.