Download
1 / 42
420 likes | 671 Views
Assisted Reproductive Technology in Resource-Poor Settings. Arlene D. Bardeguez, MD, MPH Dept. of Obstetrics, Gynecology & Women’s Health New Jersey Medical School. Definitions.

E N D
Assisted Reproductive Technology in Resource-Poor Settings Arlene D. Bardeguez, MD, MPH Dept. of Obstetrics, Gynecology & Women’s Health New Jersey Medical School
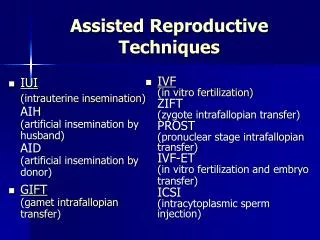
Definitions • Assisted Reproductive Technologies (ART) include all fertility treatments in which both eggs and sperm are handled. FCSRCA Publication # 102-493, October 24, 1992.
Reproductive Options for HIV-infected Women: Historical Perspective USA • 1985 Recommendation from CDC: Women known to be HIV(+) should defer pregnancy • concerns disease progression • concerns lethality of disease • concerns of risk perinatal transmission • 1990 CDC Reported that Use of Assisted Reproductive Technologies could lead to horizontal transmission
Reproductive Options for HIV-infected Women: Historical Perspective • 1994: Use of antiretroviral therapy and/or operative delivery lead to a dramatic decrease in perinatal HIV-1 transmission • 1996: Introduction of HAART in clinical practice • decrease mortality • increase life-span • increase pool of individuals with stable HIV disease • decrease Perinatal HIV-1 Transmission
Advocates for use of assisted reproductive technologies in HIV-1 infertile couples
Perinatal HIV-1 Transmissionin the HAART Era Perinatal HIV-1 Transmission Rate @ABardeguez
Mode of Delivery and the Riskof Perinatal HIV-1 Transmission[Meta-Analysis NEJM 1999]
Patient’s Autonomy Fetal Beneficence
Opponents on the use of assisted reproductive technologies in HIV-1 infertile couples
Other arguments • Lack of Perinatal transmission can’t be guaranteed • Horizontal transmission risk of available procedures is uncertain [1st do no harm] • Overall cost of Intervention • Individual • Society
Risk/Benefits of Assisted Reproductive Technologies in HIV-Infected Subjects • Could decrease the risk of horizontal transmission for discordant couples • decrease risk of unprotected intercourse • increase conception rate [25% cycle 35% IVF] • Use of reproductive technologies can increase perinatal risk • preterm labor • low birthweight • Could increase morbidity if operative interventions are needed • Increase cost of the interventions?
Assisted Reproductive Technologies should not be denied to HIV-infected couples solely on the basis of their positive serostatus Committee on Ethics of ACOG 2001 American Society for Reproductive Medicine 2002
Something to Think About! By 1999, more than 97% of all ART procedures in the United States were IVF + ICSI. Fertil Steril 78:918, 2002.
Pregnancy Rates According to Procedure Used 1 Guzick, et al., N Engl J Med 340:177, 1999. 2 Fertil Steril 78:918, 2002.
COST • IVF cycle (1 cycle): $9,226.00 • SO-IUI (1 cycle): $1,800.00 • SO-IUI (4 cycles): $7,200.00 Semin Reprod Med 331:244, 1994. Fertil Steril 67:830, 1997.
Multiple Gestations per IVF Retrievals-US 1999 Fertil Steril 78:918, 2002.
Assisted Reproductive Technology for Men and Women Infected with Human Immunodeficiency Virus Type 1 Clinical Infectious Diseases 2003; 36: 195-200 January 15, 2003
Case Scenario 1: HIV-Infected Female & Negative Male Partner • Goals • Prevent horizontal transmission • Artificial insemination with/without ovarian stimulation • Donor Insemination • IVF • Prevent perinatal transmission • Infertility work-up if needed • Anovulation [PCO, Substance use, Hypothalamic disorders, HIV?]
Case Scenario 2: HIV-Infected Male & Negative Female Partner Goals • Prevent horizontal transmission • Cell associated and cell free virus can be source of infection • There is a relation between serum and genital viral load but imperfect! • Techniques used • Intrauterine insemination after “Sperm wash” • Intracytoplasmic Sperm Injection [ICSI] • Oocyte donation
Bedford Research Foundation* Special Program of Assisted Reproduction-SPAR Pregnancies and Births as of January 2005 • 39 pregnancies have been achieved through SPAR and IVF, procedures, 6 are ongoing. • 3 pregnancies and 3 births have been achieved using the new Oligospermic Cup procedure, both are ongoing. • 26 babies have been born using SPAR and IVF procedures • 5 sets of twins • 16 singletons *Formerly Duncan Holly Biomedical Inc.
Intrauterine insemination after “Sperm wash” • Semprini et al • Over 1,000 IUI in 350 discordant couples • 200 pregnancies • No horizontal transmission • Marina et al • 63 HIV+ men without AIDS • + HIV RNA 5.6% samples [discarded] • 49% success IUI, 37 children • All women HIV(-) 6 months after IUI
Intracytoplasmic Sperm Injection [ICSI] • Sauer et al Complications • Multiple pregnancies • Ovarian stimulation syndrome • Sauer 1997-2002 • 25 couples conceived 27 pregnancies • 40 neonates • C/S rate 70% • Mean gestational age at delivery 37 weeks • 7 cases Preterm delivery • 8 cases low birth weight
Case Scenario 3: Both partners HIV-Infected • Risk/Benefits? • Optimal Management? • Options • IUI • ICSI • Oocyte Donation • Adoption
Laboratory Issues • Sample processing • Sperm washing • DNA/RNA testing • Prevent Cross-contamination • Timing procedures • Separate freezers for storage • Liquid nitrogen vapors
Criteria and Recommendations for Use of Assisted Reproductive Technologies-I • Disclosure of serostatus between partners • Pre-conceptional Counseling • Informed consent [risk, benefits, alternatives explained] • Absence of OI or prophylaxis • CD4>350cells/mm3, HIVRNA <50,000 copies/ml • Normal pap and/or colpo if abnormal • If Hepatitis C+: • normal liver enzymes • hepatology consult
Criteria and Recommendations for Use of Assisted Reproductive Technologies-II Patients receiving HAART: • HIV RNA<400 copies/ml • Regimen without teratogenic drugs • Adequate tolerance to regimen • No toxicities • Adequate response to regimen [CD4, VL] at least 1 year • Semen analysis by HIV PCR prior to insemination/IVF
Criteria and Recommendations for Use of Assisted Reproductive Technologies-III • Intrapartum ZDV prophylaxis • Close follow-up during pregnancy and after birth by HIV experts • Follow-up of child and HIV negative partner after procedure/delivery to verify lack of transmission
Optimal procedures Sperm washing Drug penetration Ethics:Risk/Benefits Access Optimal candidates Access Attitudes/Beliefs Education Patients Technology Outcomes Data collection Monitor outcomes Modify Approaches based on evidence Financial Support
Treatment started if Cd4<350 or viral load >100,000 Unlimited regimens Access to HAART during pregnancy Access to Intrapartum ZDV C/S done routinely Treatment started id AIDS or CD4<200 Preferred options for treatment HAART access limited women with advance disease NEV used intrapartum Limited access to C/S Contrast between US orInternational Guidelines, Access to Care
Technology Transfer fromDevelop to Under-develop Countries: Cost, Simplicity • Insemination – Sperm Wash • Oligo-spermic cap-Sperm Wash • IVF • ICSI
Ideal Candidate-Individual • Committed couple • Younger couple • No STI’s • Able to use post-exposure prophylaxis • Cultural beliefs will not hinder condom use during pregnancy • Able to not breastfeed postpartum • Will have access to treatment if disease progress
Ideal Candidate-Community • Access to treatment prior to AIDS diagnosis: diversity of options • Access to IV ZDV in labor or effective antiretroviral for MTCT • Timely and safe access to C/S • Access to neonatal antiretrovirals for MTCT prevention and follow up • Long term assessment-cost to society
Ideal Candidate-Site • Assisted reproduction technologies on site • Quality control assessment • Ongoing training • Culturally acceptable • Criteria for qualification not link to patient’s resources
Unknowns!! • Cost effectiveness of averting horizontal and perinatal transmission versus cost intervention • Will current technology for sperm wash be equally effective all clades • Ethics of limiting access to younger population based on fertility rate and life potential • Should access be limited to 1 pregnancy per couple