Download
1 / 9
90 likes | 1.04k Views
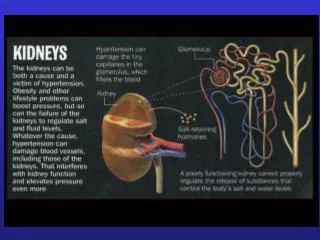
ESA Dose Adjustment in Dialysis Patients: Implications for ESA Prescribing Information. Robert Provenzano, MD DaVita. Cohort-1 (Hb 12-13g/dl) Hemodialysis Patients Hb 12-13 g/dL end of month, December 2006 Level of dose decrease in January 2007 10-25%, 26-50%, 51-99%, or 100%

E N D
ESA Dose Adjustment in Dialysis Patients: Implications for ESA Prescribing Information Robert Provenzano, MD DaVita
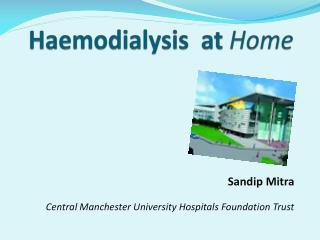
Cohort-1 (Hb 12-13g/dl) Hemodialysis Patients Hb 12-13 g/dL end of month, December 2006 Level of dose decrease in January 2007 10-25%, 26-50%, 51-99%, or 100% Follow month-to-month Hb changes through June 2007 Cohort-2 (Hb >13g/dl) Hemodialysis Patients Hb > 13 g/dL end of month, December 2006 Level of dose decrease in January 2007 10-25%, 26-50%, 51-99%, or 100% Follow Hb changes through June 2007 Relationship between degree of dose reduction and Hb outcomes in patients with initial Hb 12-13 g/dL or Hb > 13 g/dL
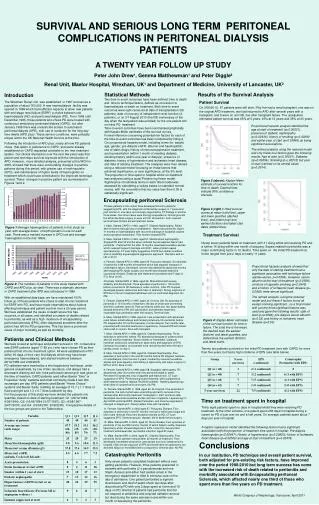
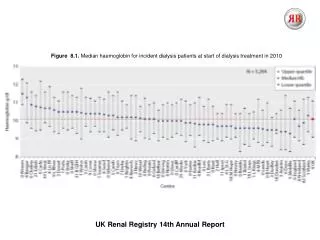
Holding Epoetin alfa when Hb is 12-13 g/dL increases relative risk of both low Hb early and high Hb later Source: DaVita internal data
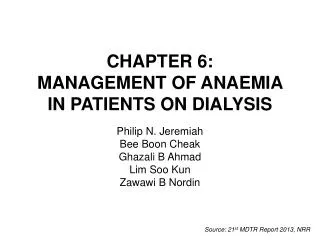
Holding at Hb > 13 increases risk of Hb < 11 early, > 13 late Source: DaVita internal data
Larger epoetin dose reductions are associated with higher epoetin dose requirements Source: Data from Thamer M et al. JAMA 297 (15):1667-1674, 2007, Table 2.
Better anemia management is also associated with higher epoetin dose requirements Source: Data from Thamer M et al. JAMA 297 (15):1667-1674, 2007, Table 2.
Trend in Standardized Mortality Ratio (SMR) for all Dialysis Patients, 1985-2002 -19%
AdministerEPOGEN® at the lowest dose needed to achieve a hemoglobin > 11g/dL. Decrease the EPOGEN® dose if the hemoglobin exceeds 12g/dL or the hemoglobin rate of rise exceeds 1g/dL per two weeks or 2g/dL per 4 weeks.
Conclusions • Create Policies & warning specific to the CKD/ESRD population • Do not encourage withholding epoetin alfa as standard practice or making large dose decreases for Hb values above target: • Dangerous • Increases risk of early, serious anemia • Counterproductive • Increases risk of later, above-target Hb • May increase epoetin utilization • Current CMS regulations and Clinical Performance Measures • Are safe, sufficient, and well-supported by evidence • Do not underestimate or undervalue QOL…