Download
1 / 51
510 likes | 1.03k Views
1 case - Macau*, Kuwait, Ireland, Romania, Russian Federation, Spain, Switzerland and South Korea. UK no ... advised against all but essential travel to Toronto, noting that a ...

E N D
Slide 1: SARS CoV - The first major Pandemic of the third Millenum - Lessons to Learn!
John W Hartley - CMS Secretariat Truro Where I have taken images from the Internet or elsewhere I have indicated the source on the slide. Alternative Title - The Story of SARS Alternative Title � SARS � a Reflection Alternative Title � SARS - A Pandemic in the age of Digital Communication Alternative Title � SARS � If you get it wrong it comes back and hits you in the Head! Alternative Title � SARS � The answer my friend is blowing in the Wind? What is interesting is that the title I started with is the title that has been retained.Where I have taken images from the Internet or elsewhere I have indicated the source on the slide. Alternative Title - The Story of SARS Alternative Title � SARS � a Reflection Alternative Title � SARS - A Pandemic in the age of Digital Communication Alternative Title � SARS � If you get it wrong it comes back and hits you in the Head! Alternative Title � SARS � The answer my friend is blowing in the Wind? What is interesting is that the title I started with is the title that has been retained.
2Slide 2:The First Clue
27 November 2002 � Canada�s Global Public Health Intelligence Network (GPHIN), an electronic warning system which is part of the World Health Organization�s (WHO) Global Outbreak & Alert Response Network (GOARN), picked up reports of a �flu outbreak� in China through internet media monitoring & analysis and sent them to the WHO. GPHIN at that time had been updated and was capable of scanning media sources in the WHO official languages � Arabic, Chinese, English, French, Russian & Spanish. However, the GPHIN system could not accommodate the presentation of information in the other languages beside English and French. GPHIN Analysts therefore translated only the titles of selected non � English articles. ^ a b Mawudeku, A. and Blench, M. "Global Public Health Intelligence Network," mt-archive, 2005 (http://www.mt-archive.info/MTS-2005-Mawudeku.pdf) The prototype GPHIN was developed in 1997 in partnership with WHO and could only scan and report in English & French. Global media sources included websites, news wires, local and national newspapers. GPHNI was updated in 2004 and is now multilingual. In some areas of Healthcare Canada is a world leader. It is a vast country with a relative small population 31 million. It is a leader in electronic Healthcare Education such as Presentations given by PowerPoint. As Canada is a bilingual country it has a natural lead in the development of electronic Global Public Health NetworksThe prototype GPHIN was developed in 1997 in partnership with WHO and could only scan and report in English & French. Global media sources included websites, news wires, local and national newspapers. GPHNI was updated in 2004 and is now multilingual. In some areas of Healthcare Canada is a world leader. It is a vast country with a relative small population 31 million. It is a leader in electronic Healthcare Education such as Presentations given by PowerPoint. As Canada is a bilingual country it has a natural lead in the development of electronic Global Public Health Networks
3Slide 3:Concealed Information
The first case of SARS originated in Shunde, Foshan, Guandong in Nov 2002, and the patient, a farmer, was treated in the First People�s Hospital of Foshan ( McKay Dennis). The patient died soon after, and no definitive diagnosis was made on the cause of death. Despite taking some action to control it, Chinese government officials did not inform the World Health Organization of the outbreak until February 2003. This lack of openness caused delays in efforts to control the epidemic, resulting in criticism of the People�s Republic of China (PRP) from the international community. The PRC has since officially apologised for early slowness in dealing with the SARS epidemic. In the talk to help distill out what I am trying to say the points/paragraphs in purple focus on major learning points.In the talk to help distill out what I am trying to say the points/paragraphs in purple focus on major learning points.
4Slide 4:Red Herrings
WHO requested information from Chinese authorities on December 5 & 11. On December 12, WHO received a detailed report on data collection at Chinese influenza surveillance sites indicating that investigation of 23 influenza virus isolates had confirmed type B strains in all but one and that the number of cases was consistent with the seasonal pattern in previous years. The information was reassuring. The first English report was January 21, 2003. This was a financial report about a pharmaceutical company�s increased sales of antivirals in the Guangdong Province, Mainland China. The report attributed the increased sales to the unusual outbreak occuring in that region. On February 20 with growing concern the Hong Kong authorities confirmed the detection of A (H5N1) avian influenza virus in two persons. On March 15, 2003 a global alert was given by WHO. WHO reported 150 suspected new cases from several geographical areas, including Hong Kong, Singapore, Vietnam & Canada. The WHO also provided a name and case definition. ^ a b Heymann, D. L., and Rodier, G. "Global Surveillance, National Surveillance, and SARS," Emerging Infectious Diseases - Medscape, February 12 2004 Although information is incomplete, retrospective case identification by Chinese and Global Alert and Response Network (GOARN) epidemiologists since May 2003 suggests that two respiratory disease outbreaks in Guangdong Province in late November 2002: influenza and a first wave of SARS cases - atypical pneumonia characterised by small, seemingly unrelated clusters of cases over several municipalities in Guangdong, with low � level transmission to healthcare workers. This first wave of atypical pneumonia appears to have continued until a second wave of disease with amplified transmission to health workers began occuring during the first 10 days of February. Although information is incomplete, retrospective case identification by Chinese and Global Alert and Response Network (GOARN) epidemiologists since May 2003 suggests that two respiratory disease outbreaks in Guangdong Province in late November 2002: influenza and a first wave of SARS cases - atypical pneumonia characterised by small, seemingly unrelated clusters of cases over several municipalities in Guangdong, with low � level transmission to healthcare workers. This first wave of atypical pneumonia appears to have continued until a second wave of disease with amplified transmission to health workers began occuring during the first 10 days of February.
5 Mandell, Douglas & Bennet Principles & Practices of Infectious Disease Sixth Edition P177Slide 5: The disease spread to Hong Kong by a doctor from the mainland who arrived in February. He stayed at the Metropole Hotel infecting 16 hotel visitors. The hotel visitors spread SARS to other countries followed major airline routes. Transmission of infection occurred mainly in hospitals and among contacts and families of hospital workers. The disease spread to Hong Kong by a doctor from the mainland who arrived in February. He stayed at the Metropole Hotel infecting 16 hotel visitors. The hotel visitors spread SARS to other countries followed major airline routes. Transmission of infection occurred mainly in hospitals and among contacts and families of hospital workers.
6Slide 6:
Chu C M et al 2005 Viral load distribution in SARS outbreak. Emerg. Infect. Dis. 11 1882-1886 SARS Outbreak Amoy Gardens HKSAR Amoy Gardens is a high density middle class private housing estate comprised 19 blocks of 30-40 floors. There were 321 cases of SARS. Block E 41% of cases Block B 13% of cases Block D 13% of cases 11 other blocks 18% Possible Modes of Transmission � In most cases SARS is transmitted by direct contact with ill persons and spread of large droplets. In more distant transmission, airborne spread, contaminated fomites eg elevator door knobs or door handles, rodents & an inadequate sewage system may transmit infection. In the above study the viral load of the first 79 SARS patients from nasopharyngeal aspirates was counted using quantitative reverse transcription � polymerase chain reaction (RT-PCR). Higher nasopharyngeal viral loads were found in patients living in adjacent units of the same block inhabited by the index patient (Block E unit 7) while a lower but detectable nasopharyngeal viral load was found in patients living further away from the index patient. A northeasterly wind was blowing. The distribution pattern can be explained by airborne transmission as virus-laden aerosols were driven from Block E to blocks D, C and B. Patients living in Block D had a lower viral load than those in blocks B and C even though they lived closest to the index patient. They may have been protected by a nearby construction site which created a shield against the virus-laden draft. Concerned citizens in Hong Kong worried that information was not reaching people quick enough created a webpage called sosick.org, eventually forcing the Hong Kong government to provide information related to SARS in a timley manner. SARS Outbreak Amoy Gardens HKSAR Amoy Gardens is a high density middle class private housing estate comprised 19 blocks of 30-40 floors. There were 321 cases of SARS. Block E 41% of cases Block B 13% of cases Block D 13% of cases 11 other blocks 18% Possible Modes of Transmission � In most cases SARS is transmitted by direct contact with ill persons and spread of large droplets. In more distant transmission, airborne spread, contaminated fomites eg elevator door knobs or door handles, rodents & an inadequate sewage system may transmit infection. In the above study the viral load of the first 79 SARS patients from nasopharyngeal aspirates was counted using quantitative reverse transcription � polymerase chain reaction (RT-PCR). Higher nasopharyngeal viral loads were found in patients living in adjacent units of the same block inhabited by the index patient (Block E unit 7) while a lower but detectable nasopharyngeal viral load was found in patients living further away from the index patient. A northeasterly wind was blowing. The distribution pattern can be explained by airborne transmission as virus-laden aerosols were driven from Block E to blocks D, C and B. Patients living in Block D had a lower viral load than those in blocks B and C even though they lived closest to the index patient. They may have been protected by a nearby construction site which created a shield against the virus-laden draft. Concerned citizens in Hong Kong worried that information was not reaching people quick enough created a webpage called sosick.org, eventually forcing the Hong Kong government to provide information related to SARS in a timley manner.
7Slide 7:SARS Outbreak Amoy Gardens HKSAR
Amoy Gardens blocks standing behind a block (green colour) - Wikipedia Amoy Gardens - Cinema on the ground floor - Wikipedia Car Park entrance to Amoy Plaza shopping mall - Wikipedia Restaurants in the food square - Wikipedia Epidemiological analysis, experimental studies and airflow simulations support the possibility of an airborne spread of the SARS virus in the outbreak in Amoy Gardens. Virus-laden aerosols generated in the vertical soil stack of unit 7 in building E returned to the bathroom through the dried-up seals of the floor-drain traps and then entered the air shaft, probably by means of suction created by an exhaust fan. The aerosols moved upward owing to the buoyancy of the warm, humid air within the air shaft and could enter apartment units that bordered the air shaft on the upper floors because of the negative pressure created by the exhaust fans or the action of wind flows around the building. The horizontal spread of infection to other units in building E was by movement of air between apartment units. After the plume reached the top of the air shaft in building E, the virus appears to have been spread to some units at certain heights in buildings B, C, and D by the action of the prevailing wind. Ignatius T.S. et al Evidence of Airborne Transmission of the Severe Acute Respiratory Syndrome Virus N Engl J Med 350; 17 1731-1739Epidemiological analysis, experimental studies and airflow simulations support the possibility of an airborne spread of the SARS virus in the outbreak in Amoy Gardens. Virus-laden aerosols generated in the vertical soil stack of unit 7 in building E returned to the bathroom through the dried-up seals of the floor-drain traps and then entered the air shaft, probably by means of suction created by an exhaust fan. The aerosols moved upward owing to the buoyancy of the warm, humid air within the air shaft and could enter apartment units that bordered the air shaft on the upper floors because of the negative pressure created by the exhaust fans or the action of wind flows around the building. The horizontal spread of infection to other units in building E was by movement of air between apartment units. After the plume reached the top of the air shaft in building E, the virus appears to have been spread to some units at certain heights in buildings B, C, and D by the action of the prevailing wind. Ignatius T.S. et al Evidence of Airborne Transmission of the Severe Acute Respiratory Syndrome Virus N Engl J Med 350; 17 1731-1739
8Slide 8:Death of Health Care Worker Dr Carlo Urbani
Dr Carlo Urbani an Infectious Disease Specialist was employed by WHO and based in Hanoi, Vietnam attends Johnny Chen Dr Urbani notifies the WHO of a probably new and contagious infection. Carlo Urbani contracts the illness and dies March 29 2003 Dr Carlo Urbani Source -Wikipedia http://en.wikipedia.org/wiki/Carlo_Urbani In February 2003 the disease reached the public spotlight. An American businessman Johnny Chen travelling from China developed pneumonia � like symptoms while on a flight to Singapore. The plane stopped in Hanoi, Vietnam, where the victim died in the French Hospital of Hanoi. Dr Urbani started to feel feverish while flying to Bangkok where he planned to speak on the subject of childhood parasites. At the airport a colleague met him and called an ambulance. They sat in chairs 8 feet apart until an ambulance arrived 90 minutes later. It�s attendants had stopped first for protective gear. He was isolated in hospital and his wife was only allowed to speak to him by intercom. In a conscious moment he asked for a priest to give him the last rite. According to the Italian Embassy in Bangkok, he said he wanted his lungs saved for science. In February 2003 the disease reached the public spotlight. An American businessman Johnny Chen travelling from China developed pneumonia � like symptoms while on a flight to Singapore. The plane stopped in Hanoi, Vietnam, where the victim died in the French Hospital of Hanoi. Dr Urbani started to feel feverish while flying to Bangkok where he planned to speak on the subject of childhood parasites. At the airport a colleague met him and called an ambulance. They sat in chairs 8 feet apart until an ambulance arrived 90 minutes later. It�s attendants had stopped first for protective gear. He was isolated in hospital and his wife was only allowed to speak to him by intercom. In a conscious moment he asked for a priest to give him the last rite. According to the Italian Embassy in Bangkok, he said he wanted his lungs saved for science.
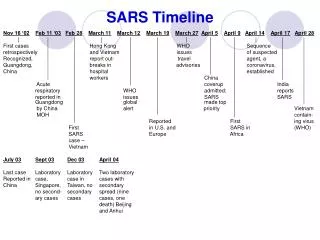
9Slide 9: Probable cases of SARS by Country, 1 Nov 02 � 31 July 03
(*) Figures for the People�s Republic of China exclude the Special Administrative Regions (Macau, SAR, Hong Kong SAR) which are reported separately by the WHO. (**) Since 11 July 2003, 325 Taiwanese cases have been �discarded�. Laboratory information was insufficient or incomplete for 135 discarded cases: 101 of these patients died. 1 case - Macau*, Kuwait, Ireland, Romania, Russian Federation, Spain, Switzerland and South Korea UK � no cases 6 major sites affected and 20 additional sites ^ a b c Epidemic and Pandemic Alert and Response (EPR), World Health Organization (WHO) (http://www.who.int/csr/sars/country/en/index.html) Lesson � The Taiwanese experience demonstrates how important it is to complete accurate documentation and return it to the appropriate National/International Surveillance Agency. Lesson � The Taiwanese experience demonstrates how important it is to complete accurate documentation and return it to the appropriate National/International Surveillance Agency.
10Slide 10: South West Laboratory Reports Received in LabBase by Laboratory, from 01/06/2009 to 31/08/2009 with Reporting Timeliness
16 reporting laboratories - % return within 21 days One laboratory failed to achieve a 50% return Six more laboratories failed to achieve a 90% return Nine laboratories achieved > 90% South West 88% England, Wales & N. Ireland 73% Health Protection Agency
11 Jernigan JA, Low DF, Heifand RF. Combining clinical and epidemiolgical features for early recognition of SARS. Emerg Infect Dis 2004: 10: 327-333.Slide 11:The C � Reactive protein is slightly raised.The C � Reactive protein is slightly raised.
12Slide 12:Chest x-ray
Chest x-ray in a patient with SARS - Wikipedia Note the ground � glass opacities and focal consolidation, especially in the periphery and subpleural regions of the lower zones.Note the ground � glass opacities and focal consolidation, especially in the periphery and subpleural regions of the lower zones.
13Slide 13:Unusual Features of SARS
Few cases of illness were recognised or reported in children A high proportion of cases occurred in health care workers. In the five most affected locations, 20% of all cases were observed in health care workers The transmission dynamics were highly variable. Most individuals appeared not to transmit the disease to other persons
14Slide 14:Unusual Features of SARS - Superspreaders
In certain situations infected individuals were linked to a large number of subsequent cases The basis for the super-spreader phenomen is unknown Possible hypotheses include Host or environmental factors Virus burden Coinfection Coinfection & medical interventions that may have widely aerosolized the virus
15Slide 15: Various Settings for Transmission
Inpatient & Outpatient health care settings Hotels Apartment Complexes Conveyances (airplanes, trains & taxicabs) Religious gatherings The community In most of these settings, close, direct contact appeared to be the most important factor associated with disease transmission, suggesting that droplet or fomite transmission was the predominant mode of spread. The role of alternative modes of transmission, particularly aerosols and environmental contamination, is less clear but best fits disease patterns in certain settings. No evidence supports foodborne or blood-borne transmission of SARS coronavirus.In most of these settings, close, direct contact appeared to be the most important factor associated with disease transmission, suggesting that droplet or fomite transmission was the predominant mode of spread. The role of alternative modes of transmission, particularly aerosols and environmental contamination, is less clear but best fits disease patterns in certain settings. No evidence supports foodborne or blood-borne transmission of SARS coronavirus.
16Slide 16:Air Travel
Of a total of 40 flights investigated, 5 were associated with probable in flight SARS transmission, affecting 37 passengers Most of the affected passengers sat within five rows of the index case The overall risk of transmission appeared to be low, at around 1 in 156 Symptomatic SARS patients appeared to transmit infections on board much more readily than pre-symptomatic ones In the largest incident, during a 3 hour flight carrying 120 passengers travelling from HK Special Administrative Region (SAR) to Beijing, a superspreading event (SSE) infected 22 passengers. The pattern of involvement was atypical, considering the short duration of exposure of 3 h and the widespread involvement of patients sitting within seven rows in front and five rows behind the index case. Although airborne transmission was thought possible, other possible modes of transmission, such as contact of passengers with the index case before or after the flight, cannot be excluded, especially since 17 out of 22 people infected were from 2 tourist groups.In the largest incident, during a 3 hour flight carrying 120 passengers travelling from HK Special Administrative Region (SAR) to Beijing, a superspreading event (SSE) infected 22 passengers. The pattern of involvement was atypical, considering the short duration of exposure of 3 h and the widespread involvement of patients sitting within seven rows in front and five rows behind the index case. Although airborne transmission was thought possible, other possible modes of transmission, such as contact of passengers with the index case before or after the flight, cannot be excluded, especially since 17 out of 22 people infected were from 2 tourist groups.
17Slide 17: Morphology of the SARS coronavirus
Electron micrograph of the virus that was cultivated in Vero cells (Image courtesy of Dr L. Kolesnikova, Institute of Virology, Marburg, Germany). Nature Reviews Vol 1. Dec 2003 P209 -213 Large, club-shaped protrusions consisting of spike protein form a crown-like corona that gives the virus its nameLarge, club-shaped protrusions consisting of spike protein form a crown-like corona that gives the virus its name
18Slide 18:Schematic Representation of the Virus
A lipid bilayer comprising the spike protein, the membrane glycoprotein and the envelope protein cloaks the helical nucleocapsic, which consists of the nucleocapsid protein that is associated with the viral RNA. In the case of coronoviruses, the lipid envelope is derived from intracellular membranes Stadler K. et al. SARS - Beginning to understand a new Virus. Nature Reviews. Vol 1 Dec 2003 P209-218
19Slide 19:Genetics
Following unprecedented colloboration between laboratories and scientists worldwide, a previously unidentified coronavirus was isolated Fetal Rhesus Monkey Kidney (FRhK-4) & Vero E6 cells were inoculated with nasopharyngeal, oropharyngeal, and sputum specimens The virus genome aided by computers was sequenced at the British Cancer Agency and completed at 4 a.m. Saturday, 12 April 2003 On 16 April 2003, the WHO issued a press release stating that a coronavirus identified by a number of laboratories was the official cause of SARS At Erasmus University in Rotterdam scientists in experiments where macaques were infected with the virus developed the same symptoms as human SARS victims so fulfilling Koch�s postulates
20Slide 20:Phylogenetic tree of 28 Coronaviruses
Cheng VC et al Severe Acute Respiratory Syndrome Coronavirus as an Agent of Emerging & Reemerging Infection. Clin Micro Rev Oct 2007 Vol 20 No 4 p 660-694 Coronavirus has three groups. In Group 2b Bat SARS CoV, Civet SARS CoV and Human SARS CoV closely bunch. Coronavirus has three groups. In Group 2b Bat SARS CoV, Civet SARS CoV and Human SARS CoV closely bunch.
21Slide 21: Genomic Structure of SARS - CoV
Stadler K. et al. SARS - Beginning to understand a new Virus. Nature Reviews. Vol 1 Dec 2003 P209-218 Replication and structural regions are shown together with the predicted cleavage products in ORF1a and ORF1b. The position of the leader sequence (L), the 3� poly(A) tract and the ribosomal frameshift site between ORF1a and ORF1b are also indicated. Each box represents a protein product (Nsp, non-structural protein). Colours indicate the level of amino � acid identity with other coronaviruses. The SARS-CoV accessory genes are white. Filled circles indicate the positions of the nine transcription �regulatory sequences (TRS�s) that are specificic for SARS-CoV. Replication and structural regions are shown together with the predicted cleavage products in ORF1a and ORF1b. The position of the leader sequence (L), the 3� poly(A) tract and the ribosomal frameshift site between ORF1a and ORF1b are also indicated. Each box represents a protein product (Nsp, non-structural protein). Colours indicate the level of amino � acid identity with other coronaviruses. The SARS-CoV accessory genes are white. Filled circles indicate the positions of the nine transcription �regulatory sequences (TRS�s) that are specificic for SARS-CoV.
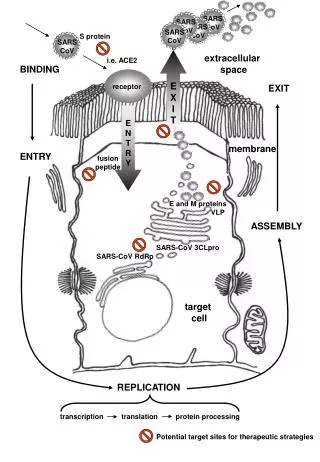
22Slide 22:Coronavirus Replication
Stadler K. et al. SARS - Beginning to understand a new Virus. Nature Reviews. Vol 1 Dec 2003 P209-218 Coronaviruses contain the largest RNA genomes described so far � the positive-sence, single-stranded RNA molecule has a 5� cap and a 3� poly(A)tail. ENTRY to the cell occurs by membrane fusion. Cleavage by virally encoded proteinases yields the components necessary to assemble the viral replication complex which synthesizes full-length negative-strand RNA. Replication takes place in the cytoplasm in a membrane-protected microenvironment and starts with the TRANSLATION of the genome to produce the viral replicase. TRANSCRIPTION involves a discontinuous RNA synthesis (template switch) during the extension of a negative copy of the subgenomic mRNAs. Nucleocapsid (N) protein and genomic RNA assemble in the cytoplasm to form the helical nucleocapsid. This core structure acquires its envelope by budding through intracellular membranes between the endoplasmic reticulum (ER) and the golgi apparatus. The membrane (M), envelope (E) and S proteins, all of which will be acommodated by the lipid layer, are transported through the ER to the budding compartment, where the nucleocapsid probably interacts with the M protein to trigger assembly. Finally the virus is released from the host cell by fusion of virion � containing vesicles with the plasma membrane.Coronaviruses contain the largest RNA genomes described so far � the positive-sence, single-stranded RNA molecule has a 5� cap and a 3� poly(A)tail. ENTRY to the cell occurs by membrane fusion. Cleavage by virally encoded proteinases yields the components necessary to assemble the viral replication complex which synthesizes full-length negative-strand RNA. Replication takes place in the cytoplasm in a membrane-protected microenvironment and starts with the TRANSLATION of the genome to produce the viral replicase. TRANSCRIPTION involves a discontinuous RNA synthesis (template switch) during the extension of a negative copy of the subgenomic mRNAs. Nucleocapsid (N) protein and genomic RNA assemble in the cytoplasm to form the helical nucleocapsid. This core structure acquires its envelope by budding through intracellular membranes between the endoplasmic reticulum (ER) and the golgi apparatus. The membrane (M), envelope (E) and S proteins, all of which will be acommodated by the lipid layer, are transported through the ER to the budding compartment, where the nucleocapsid probably interacts with the M protein to trigger assembly. Finally the virus is released from the host cell by fusion of virion � containing vesicles with the plasma membrane.
23Slide 23:Diagnostic Tests
An ELISA (enzyme linked immunosorbent assay) � reliably detects antibodies to SARS but only 21 days after the onset of symptoms An Immunofluorescent Assay � detects antibodies 10 days after the onset of disease � is labour & time intensive. Requires an immunofluorescent microscope & experienced operator Polymerase chain reaction (PCR) � detects genetic material of the SARS virus in specimens ranging from blood, sputum, tissue & stools. The PCR test so far has proven to be very specific but not very sensitive A positive viral culture from respiratory, fecal, and occasionally, urine or tissue specimens or a fourfold rise in the neutralizing antibody titre in serum samples taken upon admission and 28 days afterwards is the most definitive evidence of infection. However, both viral culture and neutralizing antibody testing require a biosafety level 3 laboratory. Most tests have never been thoroughly investigated in prospective field trials due to the short-lasting nature of the SARS epidemic. Most data comes from evaluation of stored clinical specimens. A positive viral culture from respiratory, fecal, and occasionally, urine or tissue specimens or a fourfold rise in the neutralizing antibody titre in serum samples taken upon admission and 28 days afterwards is the most definitive evidence of infection. However, both viral culture and neutralizing antibody testing require a biosafety level 3 laboratory. Most tests have never been thoroughly investigated in prospective field trials due to the short-lasting nature of the SARS epidemic. Most data comes from evaluation of stored clinical specimens.
24Slide 24:Treatment
Largely supportive with antipyretics, supplemental oxygen & ventilatory support Broad spectrum antibiotics for community-acquired pneumonia should be given pending viral confirmation Nosocomial infections as a result of prolonged intubation and the use corticosteroids should be appropriately managed Correlation between viral loads and clinical outcome suggests that suppression of viral replication by effective antiviral drugs should be key to preventing morbidity & mortality Some of the more serious damage in SARS is due to the body�s own immune system overreacting to the virus � a cytokine storm. During the 2002-2003 outbreak of SARS immodulators such as corticosteroids were used. However steroids may increase the plasma viral load and increase the risk of nosocomial infections and avascular necrosis. Steroids have been combined with ribavirin, interferon or protease inhibitors. Numerous other potential antiviral agents have been identifies using different approaches. Due to the very short time course of this epidemic and the initial lack of suitable animal models, randomised control treatment trials were difficult to organise despite finding available commercial agents. Some of the more serious damage in SARS is due to the body�s own immune system overreacting to the virus � a cytokine storm. During the 2002-2003 outbreak of SARS immodulators such as corticosteroids were used. However steroids may increase the plasma viral load and increase the risk of nosocomial infections and avascular necrosis. Steroids have been combined with ribavirin, interferon or protease inhibitors. Numerous other potential antiviral agents have been identifies using different approaches. Due to the very short time course of this epidemic and the initial lack of suitable animal models, randomised control treatment trials were difficult to organise despite finding available commercial agents.
25Slide 25:Source?
The earliest SARS patients were tracked back to their work in live animal markets in Guangdong Province, China Among the animals for sale for the table were Masked Palm Civets & Raccoon Dogs. http://itech.pjc.edu/sctag/Masked_Palm_Civet/index.htm Searching for a source of the SARS virus it was found that some of the animals were infected with coronavirus that was remarkably similar to SARS coronavirus. Further studies made it clear that although the masked palm civets were an intermediary in the infection, the virus did not originate from them. Searching for a source of the SARS virus it was found that some of the animals were infected with coronavirus that was remarkably similar to SARS coronavirus. Further studies made it clear that although the masked palm civets were an intermediary in the infection, the virus did not originate from them.
26Slide 26:Source?
Researchers in China and Hong Kong have looked at a key protein in the SARS virus life cycle. The virus attaches to ACE2 (angiotensin-converting enzyme 2) on the mammalian cell via a spike protein on the virus surface. Researchers compared the ease with which SARS-Co-V from humans could use the ACE2 enzymes from humans, palm civet and raccoon dogs. Raccoon dog - Wikipedia Xu,L et al (2009) Angiotensin converting enzyme 2 (ACE 2) from racoon dog can serve as an efficient receptor for the spike protein of severe acite respiratory syndrome coronavirus J Gen Virol 90, 2695-2703 The receptor from raccoon dogs had the greatest affinity for SARS �CoV. This identifies a second animal as an important intermediary in the evolution of SARS. Virus has also been found in ferret badgers and domestic cats. In 2005, two studies identified a number of SARS-like coronaviruses in Chinese bats. Phylogenetic analysis of the viruses indicated a high probability that SARS coronavirus originated in bats and spread to humans either directly, or through animals held in Chinese markets. The bats did not show any visible signs of disease, but are the likely natural reservoirs of SARS � like coronavirusesThe receptor from raccoon dogs had the greatest affinity for SARS �CoV. This identifies a second animal as an important intermediary in the evolution of SARS. Virus has also been found in ferret badgers and domestic cats. In 2005, two studies identified a number of SARS-like coronaviruses in Chinese bats. Phylogenetic analysis of the viruses indicated a high probability that SARS coronavirus originated in bats and spread to humans either directly, or through animals held in Chinese markets. The bats did not show any visible signs of disease, but are the likely natural reservoirs of SARS � like coronaviruses
27Slide 27:Vaccine Development
Passive immunization has been successful in establishing protection from SARS-CoV Suggest an important role for neutralizing antibody Nucleoprotein Vaccines � can induce nucleoprotein-specific cell-mediated immunity S Protein Vaccines � appear capable of inducing neutralizing antibody. Only vaccines based on the S protein protective in animal models The emergence and identification of several common and rare human coronaviruses that cause severe lower respiratory infection argues for juducious development of robust coronavirus vaccines and vector platforms.The emergence and identification of several common and rare human coronaviruses that cause severe lower respiratory infection argues for juducious development of robust coronavirus vaccines and vector platforms.
28Slide 28:Vaccine Development
Live � attenuated virus is not a good choice because of the concern about reversion to virulence or recombination with wild strains to form new wild types An inactivated whole � virus vaccine has been tested in human Chinese volunteers Showed good neutralizing antibody with little side effects Protective efficacy and immune enhancement are still unknown An inactivated SARS-CoV strain is the easiest and most likely candidate for clinical trials if SARS returnsAn inactivated SARS-CoV strain is the easiest and most likely candidate for clinical trials if SARS returns
29Slide 29:Knowledge Gaps
Molecular basis of the physical stability and transmissibility of the virus Molecular & immunological basis of pathogenesis in humans Screening tests for early or cryptic SARS cases Foolproof infection control procedures for patient care Effective antivirals or antiviral combinations The usefulness of immunomodulatory agents for late presenters An effective vaccine with no immune enhancement The immediate animal host that transmitted the virus to caged civets in the market at the beginning of the epidemic The presence of a large reservoir of SARS-CoV-like viruses in horseshoe bats, together with the culture of eating exotic mammals in southern China, is a time bomb. The possibility of the reemergence of SARS and other novel viruses from animals or laboratories and therefore the need for preparedness should not be ignored.The presence of a large reservoir of SARS-CoV-like viruses in horseshoe bats, together with the culture of eating exotic mammals in southern China, is a time bomb. The possibility of the reemergence of SARS and other novel viruses from animals or laboratories and therefore the need for preparedness should not be ignored.
30Slide 30:Sting in the Tail
On July 5 2003 WHO announced that SARS was contained From Dec 16 2003 until January 1 2004 there were 4 new cases of SARS reported in Guangzhou in Guangdong Province These were not linked to a laboratory accident 2 of 4 cases were a waitress at a restaurant in Guangzhou that served palm civets as food and a customer who ate in the restaurant a short distance from animal cages All 6 palm civets at the restaurant were positive for SARS-CoV Wang M et al SARS � CoV Infection in a Restaurant from Palm Civet Emerg Inf Dis Vol 11 No 13 Dec 2005 P1860 - 1865 All patients had a temperature > 380C, radiological evidence of pneumonia, and serological evidence of SARS infection. Fever lasted from 6 to 18 days (median 7), no mechanical ventilation was required and the clinical course of disease ranged from 21 to 24 days with full recovery. A total of 257 contacts, including 113 close contacts, of these patients were observed for 2 weeks, with no secondary transmission identified. The S gene sequence of SARS- associated coronavirus (SARS-CoV) isolated from 2 of these 4 patients was found to be closely related to the sequence of virus isolated from palm civets. One patient reported no contact with palm civets or other animals in the preceding 2 months. The remaining patient was a 20 � year-old waitress from a restaurant that served palm civet as food.All patients had a temperature > 380C, radiological evidence of pneumonia, and serological evidence of SARS infection. Fever lasted from 6 to 18 days (median 7), no mechanical ventilation was required and the clinical course of disease ranged from 21 to 24 days with full recovery. A total of 257 contacts, including 113 close contacts, of these patients were observed for 2 weeks, with no secondary transmission identified. The S gene sequence of SARS- associated coronavirus (SARS-CoV) isolated from 2 of these 4 patients was found to be closely related to the sequence of virus isolated from palm civets. One patient reported no contact with palm civets or other animals in the preceding 2 months. The remaining patient was a 20 � year-old waitress from a restaurant that served palm civet as food.
31Slide 31:Laboratory Accidents
Singapore - early September 2003 � laboratory worker became PCR positive for the SARS virus Taipei (Taiwan) � 3 months later a similar isolated laboratory became infected without secondary transmission Bejing - April 2004 � a third incident occurred involving 2 workers. One of the cases transmitted the infection to a family member and a health worker
32Slide 32:Control - Quarantine
Hong Kong � 1200 � Schools closed until 21 April. Singapore � 977 - Schools closed for 10 days Taiwan - 1147 Canada � thousands quarantined WHO set up a network for doctors and researchers dealing with SARS, consisting of a secure web site to study chest x-rays and a teleconference. On 27 March 2003 WHO recommended screening of airline passengers for symptoms of SARS. In Singapore, a single hospital, Tan Tock Seng Hospital, was designated as the sole treatment and isolation centre. For all confirmed and probable cases of the disease on 22 march. WHO set up a network for doctors and researchers dealing with SARS, consisting of a secure web site to study chest x-rays and a teleconference. On 27 March 2003 WHO recommended screening of airline passengers for symptoms of SARS. In Singapore, a single hospital, Tan Tock Seng Hospital, was designated as the sole treatment and isolation centre. For all confirmed and probable cases of the disease on 22 march.
33Slide 33: Control - Singapore Parliament recalled to amend the Infectious Disease Act � 24 April
Suspected persons brought to designated treatment centres + prohibited from going to public places Contaminated areas designated � access restricted � destruction of suspected sources Powers to tag offenders who break home quarantine (persons who failed to be contacted 3 times by phone consecutively) with electronic wrist tags & imposition of fines without court trial Ability to charge repeated offenders in court � may lead to imprisonment Prosecution for those lying to health officials about travel to SARS affected areas or contact with SARS patients In Singapore, a single hospital, Tan Tock Seng Hospital, was designated as the sole treatment and isolation centre for all confirmed and probable cases of the disease on 22 March. All staff submitted to temperature checks twice a day, visitors were restricted only to pediatric, obstetric and selected other patients. Only one person was allowed to visit at a time. To overcome the inconvenience videoconferencing was utilised. A dedicated phoneline was designated to report SARS cases, whereupon a private ambulance service was dispatched to transport to Tan Tock Seng Hospital. On 24 March, Singapore�s Ministry of Health invoked the Infectious Disease Act allowing 10 day mandatory home quarantine on all who had contact with SARS patients. SARS patients discharged from hospitals were under 21 days home quarantine, with telephone surveillance requiring them to randomly answer the phone when called up. Home quarantine was imposed for 14 days on discharged probable SARS patients and some recovered cases of suspected SARS patients. Security officers from CISCO, a Singaporean auxilary police force, were utilised to serve quarantine orders to their homes, and installed an electronic picture camera (ePIC) outside the door of each contact. The recall of Parliament was sparked by an elderly gentleman who disregarded the quarantine order, strolled to eating outlets and caused a minor exodus of patrons. On 23 April, Singapore instituted thermal imaging scans to screen all passengers departing from Singapore Changi Airport and at it checkpoints with Malaysia. Students and teachers were issued with free personal oral digital thermometers. In Singapore, a single hospital, Tan Tock Seng Hospital, was designated as the sole treatment and isolation centre for all confirmed and probable cases of the disease on 22 March. All staff submitted to temperature checks twice a day, visitors were restricted only to pediatric, obstetric and selected other patients. Only one person was allowed to visit at a time. To overcome the inconvenience videoconferencing was utilised. A dedicated phoneline was designated to report SARS cases, whereupon a private ambulance service was dispatched to transport to Tan Tock Seng Hospital. On 24 March, Singapore�s Ministry of Health invoked the Infectious Disease Act allowing 10 day mandatory home quarantine on all who had contact with SARS patients. SARS patients discharged from hospitals were under 21 days home quarantine, with telephone surveillance requiring them to randomly answer the phone when called up. Home quarantine was imposed for 14 days on discharged probable SARS patients and some recovered cases of suspected SARS patients. Security officers from CISCO, a Singaporean auxilary police force, were utilised to serve quarantine orders to their homes, and installed an electronic picture camera (ePIC) outside the door of each contact. The recall of Parliament was sparked by an elderly gentleman who disregarded the quarantine order, strolled to eating outlets and caused a minor exodus of patrons. On 23 April, Singapore instituted thermal imaging scans to screen all passengers departing from Singapore Changi Airport and at it checkpoints with Malaysia. Students and teachers were issued with free personal oral digital thermometers.
34Slide 34: Thermal imaging at Taoyuan (Taiwan) International Checkpoint
Source - Wikipedia
35Slide 35:Control - Toronto
On 23 April WHO advised against all but essential travel to Toronto, noting that a small number of persons from Toronto appear to have �exported� SARS to other parts of the world. Toronto public health officials noted that only one of the supposedly exported cases had been diagnosed as SARS and that new SARS cases in Toronto were originating in hospitals (no new cases had originated outside hospital for 20 days). All Canadian SARS cases were believed to be directly or indirectly traceable to the originated identified carriers. SARS was not loose in the community at large although a few infected persons had broken quarantine and moved among the general population. The WHO advisory was immediately followed by similar advisories by several governments to their citizens. On 29 April WHO advised that the advisory be withdrawn 30 April.
36Slide 36: Control - Summary of advice (consistent with guidance provided by HSE and WHO)
If a patient fitting the case definition for SARS is admitted to the hospital, clinicians should notify infection control personnel immediately. Until the cause and route of transmission are known, in addition to standard precautions, infection control measures for inpatients should include: Airborne precautions, eg Either an isolation room with negative pressure relative to the surrounding area or a single room with own bathroom and toilet facilities Source - http://www.hpa.org.uk
37Slide 37: Control - Summary of advice (consistent with guidance provided by HSE and WHO)
Use of FFP3 filtering masks (98% filtering efficiency) conforming to EN 149:2001 for persons entering the room.�Care should be given to face-fit testing for this equipment. In the UK COSHH (and other) Regulations require that PPE shall comply with the Personal Protective Equipment Regulations (2002). Simply this means PPE shall be 'CE' marked, ie conform to the European PPE Directive (89/686/EEC). Source - http://www.hpa.org.uk
38Slide 38: Control - Summary of advice (consistent with guidance provided by HSE and WHO)
Contact and droplet precautions (including use of long sleeve fluid repellent gown and latex or similar non-latex gloves with long tight-fitting cuffs for contact with the patient or their environment) Standard precautions to include careful attention to hand washing and hygiene When caring for patients with SARS, clinicians should wear eye protection for all patient contact Standard precautions should be in place when handling any clinical waste, and must be placed in leak-proof clinical waste bags or bins and disposed of safely Source - http://www.hpa.org.uk
39Slide 39: Control - Summary of advice (consistent with guidance provided by HSE and WHO)
Laundry should be classified as infected If hospitals lack isolation facilities and lots of cases occur, then cohort nursing is recommended as per WHO guidelines Hypochlorite is the recommended disinfectant for environmental decontamination Note evidence that SARS coronavirus can survive in environment for up to 24hrs. Source - http://www.hpa.org.uk
40Slide 40:Socioeconomic Effect - China
The 2003 FIFA Women�s World Cup originally scheduled for China was moved to the USA The 2003 International Ice Hockey Federation Women�s World Championship planned to take place in Bejing was cancelled In the past rarely had officials stepped down purely because of administrative mistakes. Health Minister Zhang Wenkang was fired for irresponsibility & wrongdoing during the SARS crisis
41Slide 41:Socioeconomic Effect - China
The usually jam - packed Beijing Subway, as seen during the SARS outbreak � source Wikipedia
42Slide 42:Socioeconomic � Hong Kong
Some members of Hong Kong Legislative Council recommended editing the budget for increased spending on medical services Hong � Kong merchants withdrew from an international jewelry and timepiece exhibition in Zurich A full body check of the 1000 Hong Kong participants was enforced Merchant union leaders alleged probable racial discrimination towards Chinese merchants as the exhihibition allowed merchants to participate but not promote their own goods However exhibitors from HongKong were allowed to sell their products in their own room An estimated several hundred million HongKong dollars in contracts were lost.
43Slide 43:Socioeconomic - Taiwan
Both China & Taiwan were dealing with SARS epidemics at the same time The cross-politics inevitably complicated the way the disease was handled Since the People�s Republic of China (PRC) insisted on representing the 23 million Taiwanese people in the WHO by itself and forbade ROC�s government�s participation, Taiwan, which was one of the most endemic areas of the world, did not receive direct advice from WHO ROC claimed that lack of direct communication with the WHO precluded proper handling of the disease and caused unnecessary deaths. The PRC claimed that video conferences held between her experts and Taiwanese experts already facilitated information distribution and improved SARS treatment in Taiwan. The ROC further advocated its own seats in WHO and used the case of SARS to illustrate the importance of Taiwan included in global health monitoring. Under pressure from the PRC, Taiwan was excluded from several major SARS conferences held by WHO. WHO eventually sent experts to Taiwan to conduct inspections at the end of the SARS endemic.The ROC further advocated its own seats in WHO and used the case of SARS to illustrate the importance of Taiwan included in global health monitoring. Under pressure from the PRC, Taiwan was excluded from several major SARS conferences held by WHO. WHO eventually sent experts to Taiwan to conduct inspections at the end of the SARS endemic.
44Slide 44:Socioeconomic - Canada
In Toronto most conferences & conventions were cancelled On 22 April in Toronto the hotel occupancy rate was only half the normal rate Tour operators were reporting large declines in business The US Library of Congress officially excluded itself from attending the American Library Association convention in Toronto in summer 2003 To revitalise the city�s tourism trade The Rolling Stones and others organised the massive Molson Canadian Rocks for Toromnto concert � commonly known as SARSstock. In 2005 and 2006, The Rumoli Brothers (a comedy duo based in Toronto) put on SARSical ; a musical that explored the lighter side of the epidemic and poked fun at the media�s overreaction to the 43 deaths that occurred in Toronto.To revitalise the city�s tourism trade The Rolling Stones and others organised the massive Molson Canadian Rocks for Toromnto concert � commonly known as SARSstock. In 2005 and 2006, The Rumoli Brothers (a comedy duo based in Toronto) put on SARSical ; a musical that explored the lighter side of the epidemic and poked fun at the media�s overreaction to the 43 deaths that occurred in Toronto.
45Slide 45:Socioeconomic � United States
No SARS � related deaths 8 laboratory - confirmed cases. All contracted abroad Mainstream media fixation on possible domestic epidemic Metaphors described SARS as the product of Chinese �culture� 14% of Americans avoided Asian businesses SARS illustrated that responses to a deadly epidemic can occur far beyond the region experiencing actual infections, particularly in the age of the Internet.SARS illustrated that responses to a deadly epidemic can occur far beyond the region experiencing actual infections, particularly in the age of the Internet.
46Slide 46:New York City�s Chinatown
Rumours of local infection circulated fear around the community Many Asian Americans felt stigmatized in public SARS caused economic damage to Chinatown�s economy In the Summer of 2004, one year after SARS was contained tourism and business was still lagging Chinatown community members responded by organizing demonstrations to refute rumors of local infections. Prominent politicians such as Senator Hilary Rodham Clinton publicly dined in Chinatown restaurants Tourism plummeted. Restaurants suffered losses particularly after one rumour that a local restaurant owner had spread SARS to his employees before dying. Even without a single infection, Chinatown was quickly identified as a site of contagion and risk. The scare revealed many fissures within the Chinatown community. Some Chinese community members used events to voice concerns about sanitation, public health, and undocumented immigtants in Chinatown Tourism plummeted. Restaurants suffered losses particularly after one rumour that a local restaurant owner had spread SARS to his employees before dying. Even without a single infection, Chinatown was quickly identified as a site of contagion and risk. The scare revealed many fissures within the Chinatown community. Some Chinese community members used events to voice concerns about sanitation, public health, and undocumented immigtants in Chinatown
47Slide 47:The severe acute respiratory syndrome (SARS CoV � a coronavirus) -Summary
The epidemic � November 2002 � July 2003 -114 days Origin � People�s Republic of China Spread � to 37 countries Probable cases � 8096 Deaths � 774 � Case fatality rate 9.6% Incubation period � 2-14 days Maximum viraemia � 10 days after onset
48Slide 48: The severe acute respiratory syndrome (SARS CoV � a coronavirus) - Summary
Period of communicability � Not completely understood. Initial studies suggest transmission does not occur before onset of clinical signs and symptoms, and that maximum period of communicability is less than 21 days. Health workers are at great risk, especially if involved in pulmonary procedures such as intubation or nebulization. Mortality with age 24 or <: 1%. 25-44: 6%. 45-64: 15% >65: 50%
49Slide 49: The severe acute respiratory syndrome (SARS CoV � a coronavirus) - Summary
Now contained Not claimed to be eradicated (unlike smallpox) as it may still be present in its natural host reservoirs (animal populations) SARS-CoV is one of 36 coronaviruses in the family Coronaviridae within the order Nidovirales
50Slide 50: What can we Learn for future Pandemics?
Multilingual communication is essential Concealing information will endanger lives Good quality reporting from laboratories to National/International Surveillance Agencies is essential The Red Herrings Risks to Health Care Workers Good advice from National/International Organisations Good relationships between countries The rumour mill In some areas of Healthcare Canada is a world leader. It is a vast country with a relative small population of 31 million. It is a leader in electronic Healthcare Education such as Presentations given by PowerPoint and Teleconference. As Canada is a bilingual country it has a natural lead in the development of electronic Global Public Health Networks. During the SARS epidemic Canada�s Global Public Health Intelligence Network (GPHIN) could scan electronic media in the 6 WHO languages Arabic, Chinese, English, French, Russian & Spanish. However, it could only report in English and French. The system has now been updated to report in all 6 WHO languages. Despite taking some action to control it, Chinese government officials did not inform the World Health Organization of the outbreak until February 2003. This lack of openness caused delays in efforts to control the epidemic, resulting in criticism of the People�s Republic of China (PRC) from the international community. The PRC has since officially apologised for early slowness in dealing with the SARS epidemic. 325 Taiwanese cases have been �discarded�. Laboratory information was insufficient or incomplete for 135 discarded cases: 101 of these patients WHO requested information from Chinese authorities on December 5 & 11. On December 12, WHO received a detailed report on data collection at Chinese influenza surveillance sites indicating that investigation of 23 influenza virus isolates had confirmed type B strains in all but one and that the number of cases was consistent with the seasonal pattern in previous years. The information was reassuring. On February 20 with growing concern the Hong Kong authorities confirmed the detection of A (H5N1) avian influenza virus in two persons. Carlo Urbani contracts the illness and dies March 29 2003 The WHO directive to avoid travel to Toronto which seems at odds to the advise of experts in Toronto. It is cruicial to listen to the experts on the ground. War and cold wars cause epidemic disease and death The stigmatisation of Asian Americans and the impact on business in New York Chinatown was absolutely amasing. In some areas of Healthcare Canada is a world leader. It is a vast country with a relative small population of 31 million. It is a leader in electronic Healthcare Education such as Presentations given by PowerPoint and Teleconference. As Canada is a bilingual country it has a natural lead in the development of electronic Global Public Health Networks. During the SARS epidemic Canada�s Global Public Health Intelligence Network (GPHIN) could scan electronic media in the 6 WHO languages Arabic, Chinese, English, French, Russian & Spanish. However, it could only report in English and French. The system has now been updated to report in all 6 WHO languages. Despite taking some action to control it, Chinese government officials did not inform the World Health Organization of the outbreak until February 2003. This lack of openness caused delays in efforts to control the epidemic, resulting in criticism of the People�s Republic of China (PRC) from the international community. The PRC has since officially apologised for early slowness in dealing with the SARS epidemic. 325 Taiwanese cases have been �discarded�. Laboratory information was insufficient or incomplete for 135 discarded cases: 101 of these patients WHO requested information from Chinese authorities on December 5 & 11. On December 12, WHO received a detailed report on data collection at Chinese influenza surveillance sites indicating that investigation of 23 influenza virus isolates had confirmed type B strains in all but one and that the number of cases was consistent with the seasonal pattern in previous years. The information was reassuring. On February 20 with growing concern the Hong Kong authorities confirmed the detection of A (H5N1) avian influenza virus in two persons. Carlo Urbani contracts the illness and dies March 29 2003 The WHO directive to avoid travel to Toronto which seems at odds to the advise of experts in Toronto. It is cruicial to listen to the experts on the ground. War and cold wars cause epidemic disease and death The stigmatisation of Asian Americans and the impact on business in New York Chinatown was absolutely amasing.
51 INAUGURAL POWERPOINT TELECONFERENCE (PPT) OF THE CORNISH MICROBIOLOGICAL SOCIETY (COWETHAS CORBRYVYAS KERNOW) TUESDAY 12th DECEMBER 2006 Teleconference Controller - Will Gothard Lead - John Hartley Title - Risk Management of Health Care Associated Infections Delegates - Louise Rosen, Mike Cadwell, Ann Cunningham, Deborah Wadham, Vanessa Perks, Elizabeth West, Julian Rogers, Richard Bendall, Lindsey Vincent, Barrie Durant, Natasha Allen, Vic Ellis and by telephone link with the Cornwall Health Protection Unit (Saint Austell) and Brian GuttridgeSlide 51:The first CMS teleconference was Tuesday 12 December 2006. I led the conference and the conference controller was Will Gothard. Tomorrow Will leaves to take up a new post as Director of Operations at the Health Protection Agency Laboratory, Bristol. We wish him well. Will has been a great teleconference enthusiast over the years. We would like to thank him for all the work he has done to make it a success. Please receive this plaque depicting the first teleconference as a mark of our gratitude. The first CMS teleconference was Tuesday 12 December 2006. I led the conference and the conference controller was Will Gothard. Tomorrow Will leaves to take up a new post as Director of Operations at the Health Protection Agency Laboratory, Bristol. We wish him well. Will has been a great teleconference enthusiast over the years. We would like to thank him for all the work he has done to make it a success. Please receive this plaque depicting the first teleconference as a mark of our gratitude.