Download
1 / 71
710 likes | 922 Views
بسم الله الرحمن الرحيم. SARS. S evere A cute R espiratory S yndrome. Hatami M.D. MPH 2008 (1387). تاريخچه :. آغاز همه گيري : اوّل نوامبر 2002 (دهم آذرماه 1381) پايان همه گيري : نيمه اوّل ماه آگوست 2003(اواسط مرداد ماه 1382) تعداد موارد : حدود 8422 مورد

E N D
بسم الله الرحمن الرحيم SARS Severe Acute Respiratory Syndrome Hatami M.D. MPH 2008 (1387)
تاريخچه : آغاز همه گيري : اوّل نوامبر 2002 (دهم آذرماه 1381) پايان همه گيري : نيمه اوّل ماه آگوست 2003(اواسط مرداد ماه 1382) تعداد موارد : حدود 8422 مورد وسعت همه گيري : از بيش از 30 كشور جهان به سازمان جهاني بهداشت، گزارش شده است، ميزان مرگ : 916 نفر آنان جان خود را از دست داده و ميزان كشندگي بيماري را در حدود 14 درصد اعلام كردهاند
SARS Case definition 1 – Suspect case 2 – Probable case 3 – Definitive case
1 - Suspect case (1) 1. A person presenting after 1 November 2002 (10 Aban 1381) with history of:- high fever (>38 °C)AND- cough or breathing difficultyAND one or more of the following exposures during the 10 days prior to onset of symptoms:- close contact with a person who is a suspect or probable case of SARS;- history of travel, to an affected area- residing in an affected area
Suspect case (2) 2. A person with an unexplained acute respiratory illness resulting in death after 1 November 2002, but on whom no autopsy has been performedAND one or more of the following exposures during to 10 days prior to onset of symptoms:- close contact,with a person who is a suspect or probable case of SARS;- history of travel to an affected area - residing in an affected area
2 - Probable case A suspect case with: 1- radiographic evidence of infiltrates consistent with pneumonia or respiratory distress syndrome (RDS) on chest X-ray (CXR). OR 2- autopsy findings consistent with the pathology of RDS without an identifiable cause.
Exclusion criteria A case should be excluded if an alternative diagnosis can fully explain their illness.
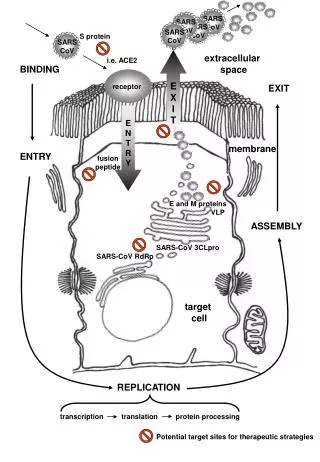
SARS Etiologic Agent • Order: Nidovirales • Family: Coronaviridae • Torovirus • Coronavirus • Grp I • Grp II • Grp III
Mode of transmission • Probable major modes of transmission • Large droplet aerosolization • Contact • Direct • Fomite • Airborne transmission cannot be ruled out • ? Role of aerosol-generating procedures • ? Fecal-oral
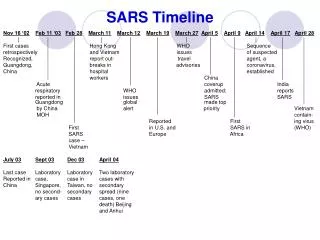
Canada 18 HCW F,G F,G 11 close contacts Ireland 0 HCW K K A Hong Kong SAR 95 HCW H,J I, L,M H,J B C,D,E I,L,M >100 close contacts C,D,E B United States 1 HCW Vietnam 37 HCW Singapore 34 HCW 21 close contacts 37 close contacts Spread from Hotel M Reported as of March 28, 2003 Guangdong Province, China A A Hotel MHong Kong
مورد اوّليه SARS (نسل اوّل) كاركنان حرفههاي پزشكي و اعضاء خانواده بيماران (نسل دوّم) اعضاء خانواده كاركنان (نسل سوّم) ساير تماس يافتگان در جامعه (نسل چهارم)
Attenuation • Attenuation is a phenomenon seen in some members of the coronavirus family, where the virulence decreases when it jumps from person to person. • The SARS virus seems to exhibit this phenomenon (however, there are no studies yet to prove this).
Viral pathogenesis - general local replication dissemination Innate cytokines phagocytes NK cells immune response end-organ involvement Adaptive primary viremia secondary viremia
Incubation Period • 2-10 days • Infected people do not pass on the virus to others during the incubation period. • They become infectious only when the first symptoms appear: cough, sneezing – which spread droplets containing virus particles.
Clinical manifestations • Incubation period 2-10 days • Onset of fever, chills/rigors, headache, myalgias, malaise • Respiratory symptoms often begin 3-7 days after symptom onset
Clinical manifestations • Sudden onset of high fever • Characteristic chest X-rays 3-4 days after onset of symptoms • 10-15% of cases require intensive care and mechanical ventilation • Case fatality about 10% • Intensive and good supportive care
Symptoms Commonly Reported By Patients with SARS1-5 Symptom Range (%) Fever 100 Cough 57-100 Dyspnea 20-100 Chills/Rigor 73-90 Myalgias 20-83 Headache 20-70 Diarrhea 10-67
Symptoms Reported by Patients With Diagnostic SARS-CoV Laboratory Testing, United States, 2003
Clinical Findings in Patients With Diagnostic SARS-CoV Laboratory Testing, United States, 2003
تشخيصهاي افتراقي SARS
برخي از عوامل مولّد پنوموني آتيپيك 1 ـ مايكوپلاسما پنومونيه 2 ـ كلاميديا پنومونيه 3 ـ كلاميديا پسيتاسي 4 ـ كوكسيلا بورنتي 5 ـ ويروسها 6 ـ پنوموسيستيس كاريني 7 ـ لژيونلائي پنوموفيلا
Diagnostic Approach to Patients with Possible SARS • Consider other etiologies • Diagnostic workup • 1 - Chest radiograph • 2 - Blood and sputum cultures • 3 - Testing for other viral pathogens (e.g. influenza) • 4 - Consider urinary antigen testing for Legionella spp. and Streptococcus pneumoniae
Diagnostic Approach to Patients with Possible SARS • 5 - Save clinical specimens for possible additional testing • Respiratory • Blood • Serum • 6 - Acute and convalescent sera (>21 days from symptom onset) should be collected • 7 - Contact Local and State Health Departments for SARS-CoV testing
Laboratory Assays for SARS • Detection of virus • EM in clinical specimens (CoV-like particles) • Isolation of virus • Detection of viral antigens • Detection of viral RNA (PCR) • Respiratory secretions • Stool specimens • Urine specimens • Tissue – lung and kidney • Detection of SARS-specific antibody • IFA • ELISA • Neutralization
Characteristics of SARS-CoV PCR • Limited experience/data • Specimens • 1 - Upper respiratory maybe ~50% positivity in acute-phase specimens • 2 - Stool possibly higher sensitivity later in illness, e.g., 10-14 days • 3 - Sputum/BAL probably higher rate of positivity • 4 - Other specimens, urine, blood, tissues, ? • Interpretation of Results • Negative -- does not rule out SARS-CoV infection • Positive – possibility of false positive (test error/contamination)
Diagnosis • SARS is a clinical and epidemiologic diagnosis • Laboratory testing can diagnose SARS-CoV infection during the acute illness • Laboratory testing can not rule out infection until the convalescent phase of illness
Radiographic Features of SARS • Infiltrates present on chest radiographs in > 80% of cases • Infiltrates • initially focal in 50-75% • interstitial • Most progress to involve multiple lobes, bilateral involvement
Treatment of Patients with SARS • Most effective therapy remains unknown • Optimize supportive care • Treat for other potential causes of community-acquired pneumonia of unknown etiology
Treatment of Patients with SARS • Potential Therapies Requiring Further Investigation • Ribavirin • ?other antiviral agents • Immunomodulatory agents • Corticosteroids • Interferons • Others?
Clinical Features Associated with Severe Disease • Older Age • Underlying illness • ? Lactate dehydrogenase levels • ? Severe lymphopenia
Infection Control • Early recognition and isolation is key • Heightened suspicion • Triage procedures • Transmission may occur during the early symptomatic phase • Potentially before both fever and respiratory symptoms develop
Treatment of Patients with SARS • Isolation • Hand hygiene • Contact Precautions (gloves, gown) • Eye protection • Environmental cleaning • Airborne Precautions (N-95 respirator, negative pressure)
Key Objectives Early detection Containment of infection Protection of personnel and the environment of care Hand hygiene Key Strategies Administrative measures Infection precautions Standard Contact (droplet) Airborne Environmental cleaning/disinfection Treatment of Patients with SARS
SARS Transmission During Aerosol-Generating Procedures • Transmission of SARS to healthcare personnel during aerosol-generating procedures may be particularly efficient • Clusters detected in Toronto, Hong Kong, Singapore and Hanoi • Intubation, suctioning and nebulization specifically implicated
Why? How? • Patient infectivity higher? • Is it: Droplet? Contact? Airborne? • Is it failure to wear protective equipment? • Is it failure of protective equipment?
Until Risks During Aerosol-Generating Procedures Better Defined….. • Limit cough-inducing procedures • Avoid use of non-invasive positive pressure ventilation (e.g., CPAP, BiPAP) • Protect the environment • Use closed suctioning devices • HEPA filtration on exhalation valve port
Protect Healthcare Personnel DuringAerosol-Generating Procedures • Limit personnel to those essential for performing procedure • Wear appropriate personal protective equipment • Gowns and gloves • Sealed eye protection (i.e., goggles) • Respiratory protection device
Respiratory Protection During Aerosol-Generating Procedures • Proper fit is essential • Reassess respirator fit among personnel who may be involved in intubation of SARS patients • Consider better fitting respiratory protection devices • Disposable respirators with better seal, e.g., N99, N100 • Half- or full-face elastomeric (rubber) • Powered air-purifying respirators (PAPR)
Management of SARS Exposures in Healthcare Settings • Surveillance of healthcare personnel • Develop list of personnel who have contact with SARS patients (I.e., enter room, participate in care) • Encourage reporting of unprotected exposures • Monitor absenteeism for SARS-like illness • Management of asymptomatic exposed HCWs
Management of Asymptomatic Exposed Healthcare Workers • No evidence of transmission from asymptomatic persons • Symptomatic HCWs have transmitted • Active surveillance of HCWs who have unprotected exposure is recommended • Monitor temperature and symptoms before reporting to duty • Ten-day exclusion from duty for HCWs who have unprotected exposures during aerosol-generating procedures
Addressing the limited supply of respirators • Should respirators be reused? • Disposal after one-time use preferred • Use up higher level respirators first • Reuse preferred to no respirator • Consider using surgical mask to protect respirator from contact with respiratory droplets • Carefully handle contaminated respirator • Use surgical masks only when respirators are unavailable