Download
1 / 30
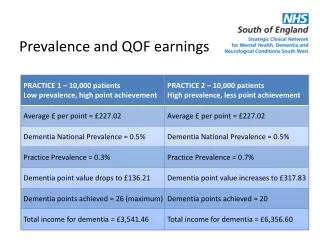
300 likes | 556 Views
Agenda. Primary care of Future/Systems ReformGMS2 and QOFBBCHA QOF analysisPossible CKD QOF indicator set. Primary Care - future. PCTContracting

E N D
1. GMS2 � QOF - ?QOF2 Dr Tony Snell
Co-Vice Chair NHS Confederation
GMS Negotiation Team
Medical Director
Birmingham and the Black Country
Strategic Health Authority
3. Limited difference between PMS & nGMS
Larger practices
More skill mix
Local variation to meet local needs
ES forces practice collaboration and multipractice consortia development
Range of other providers
Commercial companies
Not for profit organisations
Voluntary organisationsLimited difference between PMS & nGMS
Larger practices
More skill mix
Local variation to meet local needs
ES forces practice collaboration and multipractice consortia development
Range of other providers
Commercial companies
Not for profit organisations
Voluntary organisations
4. Current number of diabetics in South Gloucestershire �front - and predicted number in 10 years (almost double) � back. Ageing + illnesses affecting mainly elderly = high rise in workload.
Need to do things differently � skill-mix and concentrate on chronic disease management
Again example of changing nature
Current number of diabetics in South Gloucestershire �front - and predicted number in 10 years (almost double) � back. Ageing + illnesses affecting mainly elderly = high rise in workload.
Need to do things differently � skill-mix and concentrate on chronic disease management
Again example of changing nature
5. Pressure on NHS resources About 20% of admissions and bed-days are for patients with 3 or more unplanned admissions in a year
This group of patients (9,845 people) represents only 1 in 300 of our population, or about 7 per practice
Early intervention with these patients could have significant impact on health and hospital usage
6. Systems Changes PBR � �suck � into secondary care�
PBC � Counterweight
Secondary to primary care shift
Care closer to patient
Demand management
Referral control
Quality commissioning
?vertical integration
? Pathway development � Medic to Medic
DOCS �R� 4 US
Clinical Networks
Disinvestment strategies
7. GMS Contracts: Other PCTMS
Alternative GMS providers (APMS)
Private
Acute Trust
PMS
SPMS
Pharmacy
Dentistry
8. The contract �menu�five types of service
9. Enhanced Services National Enhanced Services
OPT-IN � national terms and conditions
�services that require specialist skills and/or facilities and/or equipment�
Anticoagulant Monitoring
Nursing Homes
IUCD
Drug and Alcohol Misuse
Local enhanced services
10. QUALITY & OUTCOMES FRAMEWORK
�A bold initiative to improve quality of care�
�With one mighty leap, the NHS vaults over anything being attempted in the United States, the previous leader in quality improvement initiatives�
Paul�Shekelle, Professor of Medicine, University of California, Los Angeles
BMJ. Vol 326, 1 March 2003: 457-8
11. The four domains of quality Clinical
Organisational
Patient experience
Additional services
12. Balance of 1000 points Clinical 550
Organisational 184
Additional Services 36
Patient Experience 100
Holistic Care 100
Quality Practice Payment 30
13. Clinical Areas CHD and LVD
Hypertension
Diabetes Mellitus
Asthma
COPD
Mental health
Stroke or TIA
Epilepsy
Cancer
Hypothyroidism 121
105
99
72
45
41
31
16
12
8
14. Principles Evidence based
Indicators fair
Clinical indicators are measurable
Not disruptive to consultation
Large explanatory document to support
15. QUALITY INDICATORS CORONARY HEART DISEASE (1)
16. QUALITY INDICATORSCORONARY HEART DISEASE (2)
17. HYPERTENSION
18. DIABETES MELLITUS (1)
19. DIABETES MELLITUS (2)
20. DIABETES MELLITUS (3)
21. Exception reporting Patients refuse to attend three times
Are new or recently diagnosed patients
It is not clinically appropriate
They have given informed dissent
They cannot tolerate medication/therapy
They are taking maximum medication
They have another supervening condition
Investigation not available to practice
22. Quality and Outcomes FrameworkAnalysis of Year End Data
24. Prevalence Map � Diabetes Mellitus
28. QOF Indicators � CHD9
29. Indicator � DM7 Indicator DM7 - The percentage of patients with diabetes in whom the last�HbA1C is 10 or less (or equivalent test/reference range depending on�local laboratory) in last 15 months.�
30. Indicator - DM7
31. Indicator � DM13 Indicator DM13 - The percentage of patients with diabetes who have a record of�micro-albuminuria testing in the previous 15 months (exception�reporting for patients with proteinuria).
32. Indicator - DM13
33. Practice List Size
34. Association with Deprivation (IMD 2004) Index of Multiple Deprivation 2004
Super Output Area
Weighted IMD score for each practice based on postcode of registrants
Correlation between QOF Score and weighted IMD
5% of variation in QOF can be explained by variations in deprivation
35. QOF and Hospital Admissions Correlation with QOF Total Score ?
Elective admission rates ?
Day Case Rates ?
Emergency Admissions ? (sig., weak, �ve,)
5% of variation in emergency admission rates explained by variations in QOF
But deprivation confounds this relationship
Sub-domain � cervical screening
36. Emergency Admissions and QOF Sub-domains
38. Chronic Kidney Disease (Draft new QOF indicator set) 1
39. Chronic Kidney Disease (Draft new QOF indicator set) 2
40. Chronic Kidney Disease (Draft new QOF indicator set) 3
41. Chronic Kidney Disease