Download
1 / 40
410 likes | 968 Views
AIDS/HIV Update. Neal R. Chamberlain, Ph.D. Associate Professor Department of Microbiology/Immunology A.T. Still University/Kirksville College of Osteopathic Medicine. Introduction- US HIV Epidemic. The HIV epidemic has claimed more than 575,000 lives

E N D
AIDS/HIV Update Neal R. Chamberlain, Ph.D. Associate Professor Department of Microbiology/Immunology A.T. Still University/Kirksville College of Osteopathic Medicine
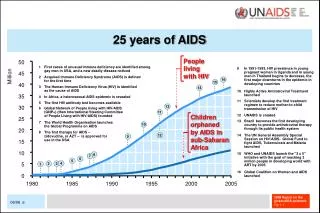
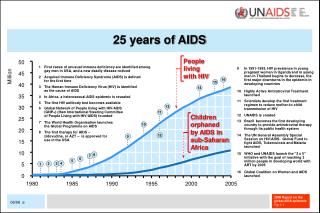
Introduction- US HIV Epidemic • The HIV epidemic has claimed more than 575,000 lives • The CDC estimates that there are from 500,000 to 1.1 million individuals living with HIV • Nearly 18,000 AIDS patients die each year • Around 56,000 new HIV infections are reported annually • Every 9 minutes and 30 seconds someone is infected with HIV http://www.cdc.gov/hiv/resources/factsheets/us.htm HIV prevalence estimates—US, 2006. MMWR 2008;57(39):1073 Hall et al. Estimation of HIV Incidence in the US. JAMA2008;300: 520
Introduction- US HIV Epidemic • 21% of the persons living with HIV do not know their HIV status (105,000-231,000 persons) • Due to the fact that they have not been tested • Higher percentages of those unaware of their HIV status were observed in high prevalence groups (MSM) • Transmission rate in undiagnosed persons is 3.5 times higher than in those that know their HIV status • The overall transmission rate is 5 per 100 person years
Introduction- US HIV Epidemic • Transmission rate in those treated with HAART is 0.46 per 100 person years • Studies of heterosexual discordant couples observed no transmission in patients treated with HAART (viral load below 400/ml) • Identifying those infected and living with HIV is essential and should significantly reduce the spread of this virus in the US
; 75% ; 25%
14% 13% 69%
Hall HI et al. Estimation of HIV Incidence in the US. JAMA 2008; 300:520
Epidemiology- Summary • Numbers of those living with HIV are increasing • Most common in those 20-45 years of age • 0ne in five don’t know they are infected with HIV • 31% diagnosed with HIV late in the infectious process • Transmission rates higher in those that don’t know they are infected • 75% of new infections are seen in males • Most common means of transmission in males: MSM • Numbers of new infections increasing in MSM • Most common means of transmission in females: heterosexual interactions • High levels of HIV infection in African American and Hispanic/Latino populations Hall et al. Estimation of HIV Incidence in the US. JAMA 2008; 300:520
Etiology • HIV-1 found worldwide- Most common in US • HIV-1 has 4 groups- M, N, O, and P • M group causes most human infections • 9 subtypes and various CRF subtypes • B subtype most common in US, Europe, and South America. • C subtype most common in sub-Saharan Africa • HIV-2 endemic in west Africa- rare cause of US infections • Retrovirus • Enveloped, diploid, single-stranded, positive-sense RNA viruses • DNA intermediate, which is an integrated viral genome (a provirus) that persists within the host-cell DNA
Transmission • Routes of infection • Sexual • Anal • Vaginal • Homosexual- most common in adult males • Heterosexual- most common in adult females • Percutaneous • Transfusions • Needle sharing • Needle stick • Maternal-child • Transplacental • Peripartum • Breast milk ingestion
Manifestations • 3 different stages • Primary HIV infection • Asymptomatic HIV infection • AIDS • Many patients are asymptomatic until stage 3 • Those infected with HIV are infectious to others in all stages • Stage 1 ends when high titers of anti-HIV antibodies are produced • Detectable levels of anti-HIV antibodies are usually observed in 2-4 weeks.
Course of Infection • Time varies by host factors and viral factors • Rapid progressors- AIDS in 2-3 yrs • Typical progressors- AIDS in 10 yrs • Long-term nonprogressors- low HIV levels; normal CD4+ T cells; >10 yrs after HIV positive • Bone marrow transplant case • Highly-exposed persistently seronegative patients- infected but no HIV antibodies or HIV-RNA detected • Disease progresses faster in certain subtypes of HIV
Pathogenesis • HIV destruction of CD4-T cells and macrophages causes immunosuppression • Killing of CD4-T cells destroys ability to mount immune response to infectious agents and to eliminate tumor cells. • More severe the disease the lower the CD4-T cell numbers and greater the amount of virus in blood stream. CJ Miller, HIV transmission: Migratory Langerhans cells are primary targets in vaginal HIV transmission Immuno Cell Biol (2007) 85:269
Diagnosis • Usually there are no unique signs or symptoms • High index of suspicion- Hx high risk behaviors, unusual infections and symptoms • Laboratory testing • Screening tests • ELISA or EIA • EIA- rapid testing (e.g., OraQuick)- can use whole blood, plasma, or oral secretions • Confirmatory tests • Western Blot analysis • RT-PCR
HIV, Surgery, and Anesthetics • Blood transfusion can cause increases in HIV viral load. Blood should be transfused only if unavoidable • Pain is common in patients with advanced HIV disease • It is multifactorial and can be difficult to treat • Opportunistic infections, HIV-related arthralgia, peripheral neuropathy, and drug-related pain • HIV infection may affect the treatment of postoperative pain • HIV infection is NOT an absolute contraindication to regional anesthesia • Certain complications associated with HIV may pose relative contraindication to regional anesthesia • Myelopathy, vertebral or spinal neoplasms, CNS infections, and coagulopathy S Wilson, HIV and Anaesthesia, 2009. Update in Anaesthesia, 25(2):25 http://update.anaesthesiologists.org/wp-content/uploads/2009/10/HIV-and-Anaesthesia.pdf
HAART Therapy CCR5 Entry Inhibitors
HAART Therapy • Selection of HAART • HAART (Highly Active Antiretroviral Therapy)- • Fewer opportunistic infections • Prolongs the life of HIV-infected patients. • Successful HAART (available since 1996) • Suppresses HIV replication. • Halts damage and partially restores the immune system and its function. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for use of antiretroviral Agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. January 10, 2011; 1-166. http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (Accessed 1/15/2011)
HAART Therapy • When to start HAART • All Pt with hx of AIDS-defining condition or CD4 T-cell count of <350 cells/mm3 • All Pt that are pregnant, HIV nephropathy, HBV co-infection when HBV Rx is needed • Recommended for all Pt with 350-500 cells/mm3 • Optional for Pt with >500 cells/mm3 Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for use of antiretroviral Agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. January 10, 2011; 1-166. http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (Accessed 1/15/2011)
HAART Therapy • Selection of HAART therapy • Treatment for naïve HIV patients • NNRTI OR a PI OR an integrase inhibitor PLUS2-NRTIs • Four regimens are now listed as “Preferred” regimens: • Efavirenz + tenofovir/emtricitabine(NNRTI+NRTI/NRTI) • Ritonavir-boosted atazanavir + tenofovir/emtricitabine (PI-PI+NRTI/NRTI) • Ritonavir-boosted darunavir + tenofovir/emtricitabine (PI-PI+NRTI/NRTI) • Raltegravir+ tenofovir/emtricitabine (integraseinhibitor+NRTI/NRTI) Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for use of antiretroviral Agents in HIV-1-infected adults and adolescents. Department of Health and Human Services. January 10, 2011; 1-166. http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf (Accessed 1/15/2011)
Therapy- Adverse effects of HAART • Four major groups • Mitochondrial dysfunction: lactic acidosis, hepatic toxicity, pancreatitis, peripheral neuropathy • Metabolic abnormalities: fat maldistribution and change in body habitus, dyslipidemia, hyperglycemia and insulin resistance, bone disorders (e.g. osteopenia, osteoporosis and osteonecrosis) • Bone marrow suppression: anemia, neutropenia and thrombocytopenia • Allergic reactions: skin rashes and hypersensitivity responses S Wilson, HIV and Anaesthesia, 2009. Update in Anaesthesia, 25(2):25 http://update.anaesthesiologists.org/wp-content/uploads/2009/10/HIV-and-Anaesthesia.pdf
Therapy- HAART and Anesthetics • Due to viral drug resistance it is recommended that HAART be continued throughout the perioperative period if at all possible • Anesthetic agents can induce pharmacodynamic changes that influence the efficacy and toxicity of HAART agents • HAART can affect the absorption, distribution, metabolism and elimination of anesthetic agents • PI’s and NNRTI’s are the most commonly implicated HAART agents associated with drug interactions • Halothane or methoxyflurane with HAART can cause hepatic or renal dysfunction • Propofol and NRTIs taken together may promote mitochondrial dysfunction and lactic acidosis S Wilson, HIV and Anaesthesia, 2009. Update in Anaesthesia, 25(2):25 http://update.anaesthesiologists.org/wp-content/uploads/2009/10/HIV-and-Anaesthesia.pdf
Therapy- HAART and Anesthetics • Opioids- • Fentanyl may be enhanced by ritonavir due to both liver enzyme inhibition and induction. Enzyme inhibition reduces fentanyl clearance and enzyme induction increases metabolism to active metabolites such as normepiridine. • Methadone clearance can be affected by some HAART agents and methadone can affect the clearance of some HAART agents • Benzodiazepines-Saquinavir may inhibit midazolam metabolism. • Local anesthetics- such as lidocaine may have increased plasma levels due to enzyme inhibition. • Neuromuscular blocker- effects may be prolonged, even a single dose of vecuronium • Calcium channel blockers- may have enhanced hypotensive effects due to enzyme inhibition. S. Wilson, HIV and Anaesthesia, 2009. Update in Anaesthesia, 25(2):25 http://update.anaesthesiologists.org/wp-content/uploads/2009/10/HIV-and-Anaesthesia.pdf
Prevention- Protecting Yourself • Screening of patients, blood supply, and of tissues to be transplanted • Do your patients know their HIV status? • Test those at low risk for HIV infection at least once in their life • Those living in areas of high HIV prevalence should be screened more frequently • Test those at high risk for HIV infection annually. Some suggest twice a year testing in high risk groups • Screen pregnant women for HIV and treat HIV positive women to prevent passage of the virus to the child • Current recommendations: treat with HAART no matter what their CD4-T cell count Vital Signs: HIV Testing and Diagnosis Among Adults- United States, 2001-2009. December 3, 2010. MMWR. 59(47): 1550
Testing Patients for HIV • Many HIV positive individuals are diagnosed late in the course of their disease (32.3%) • Transmission rates are higher in undiagnosed HIV infected persons than in those who know their HIV status • In one study it took 5 visits on average by the patient to the same healthcare facility before a dx of HIV infection was made • Recent study in JAOA- 22% of primary care DO’s recommended HIV testing to their patients during their initial visit • Osteopathic physicians who were women, African American, or Hispanic were more likely to screen patients for HIV than other DO’s. Liddicoat et al., 2004. J Gen Intern Med. 19:349 Gongidi et al., 2010. JAOA. 110:712
Testing Patients for HIV • Testing for HIV is strongly encouraged by the CDC • HIV screening is recommended for patients (13-64 years of age) in ALL health-care settings after the patient is notified that testing will be performed unless the patient declines (opt-out screening) • Annual HIV testing for individuals with high-risk behaviors • HIV screening should be included in the routine panel of prenatal screening tests for ALL pregnant women • Repeat screening in the third trimester is recommended in certain jurisdictions with elevated rates of HIV infection among pregnant women • Incorporation of permission for HIV testing into general consent forms Branson et al., 2006. MMWR. 55(RR14);1-17
Prevention- Protecting Yourself • Adopt universal infection control precautions for ALL patients • Especially if you practice in areas of high HIV prevalence • 20% of anesthesiologists had at least one needle stick injury in the past 3 months • High prevalence area; risk acquiring HIV- 4.5% during a 30yr career • Post-Exposure Prophylaxis- Know what to do in advance! • Anesthesiologists can acquire HIV during their work via: • sharp injuries (risk of HIV transmission 0.3%), • contamination of broken skin with the patients’ body fluids (risk of HIV transmission <0.1%), and • splashing HIV containing body fluid in the eyes, nose or mouth (risk of HIV transmission 0.1%) Koplan et al., 2001. MMWR. Vol. 50; RR-11 Parthasarathyet al., 2007. Ind J Anaesth. 51;91
Post-Exposure Prophylaxis • Several body fluids can transmit HIV. • They include: • Blood and fluid containing visible blood • Semen, vaginal secretions, and cerebrospinal, synovial, pleural, peritoneal, pericardial, and amniotic fluids • Human tissues can also transmit HIV • Factors which increase transmission of HIV • Hollow needle injuries • Injury by a device visibly contaminated with the patient’s blood • The injury resulted from a device placed in the patient’s vein or artery • Deep injuries • Exposure to blood from source persons with primary or terminal HIV illness Koplan et al., 2001. MMWR. Vol. 50; RR-11 Parthasarathyet al., 2007. Ind J Anesth. 51;91
Post-Exposure Prophylaxis • Clean wound with soap and water; mucosal exposures rinse with water • Report the exposure to the appropriate department (e.g., infection control, occupational health) • Start the HIV PEP regimen as soon as possible (within 2 hrs) • Treat for 4 weeks • If source is tested and found to be HIV negative discontinue PEP Branson et al., 2006. MMWR. 55(RR14);1-17
Post-Exposure Prophylaxis • Recommendations for HIV PEP include a basic 4-week regimen of 2 drugs • Zidovudine (Retrovir™) and lamivudine (Epivir™) (Combivir™ - contains both zidovudine and lamivudine), • Lamivudine (Epivir™) and stavudine (Zerit™), OR • Didanosine (Videx™) and stavudine (Zerit™) • An expanded regimen that includes the addition of a 3rd drug for HIV exposures that pose an increased risk for transmission • Indinavir (Crixivan™), Nelfinavir (Viracept™), Efavirenz (Sustiva™), or Abacavir (Ziagen™) Branson et al., 2006. MMWR. 55(RR14);1-17
Vaccines/Recent Prevention Studies • Thai vaccine study demonstrated limited success. • Immunization reduced HIV infections by around 31% • Male circumcision is associated with lower risk for HIV • May reduce male-to-female transmission; lesser extent on female-to-male transmission • Tenofovir gel for prevention of HIV infection in women • HIV incidence lowered as much as 54% in high adherence subjects; intermediate adherers (38%); low adherers (28%) • Followed for 30 months; insert gel within 12hr before sex and a second dose as soon as possible within 12hr after sex • HIV oral pre-exposure prophylaxis trial (iPrEx study) • Once daily Truvada (tenofovir and emtricitabine); Lowered risk of getting HIV in gay men and transgender women by 44% QA Karim, et al. 2010. Science. 329:1168 S. Rerks-Ngarm, et al. 2009. NEJM. 361(2):2209 RM Grant, et al. 2010. NEJM. 363(27):2587 http://www.cdc.gov/hiv/resources/factsheets/circumcision.htm