Download
1 / 67
690 likes | 896 Views
AIDS/HIV. Content. Introduction History of AIDS Prevalence Virology Immunopathogenesis Stages of AIDS HIV tests. Oral Manifestation Manifestation in children Treatment options Dental procedures at risk Universal precautions Conclusion References.

E N D
Content • Introduction • History of AIDS • Prevalence • Virology • Immunopathogenesis • Stages of AIDS • HIV tests • Oral Manifestation • Manifestation in children • Treatment options • Dental procedures at risk • Universal precautions • Conclusion • References
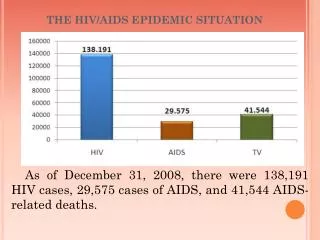
INTRODUCTION • 40 million people in 2007(W.H.O) • Two thirds present in Sub-Saharan Africa • New infections • 2.6 millions in 2004 • 4.3 millions in 2006 • 2.7 millions in 2007 • DEATH due to AIDS - 2 million in 2007. • Every 15 seconds, another person dies of HIV; every 13 seconds, another person contacts AIDS UNAIDS http://www.globalhealthreporting.org/july 2008
Person is diagnosed with AIDS when their CD4 count is below 200 & they have been diagnosed with an AIDS defining condition or an opportunistic infection • Decreased body’s ability to fight infection • Weak immune system • No Cure
Key Events In History Of HIV • Sushruta 800 b.c. and later Charaka - “loss of muscle mass, fever, skin eruption , ulcers, neurological disorders, exhaustion, coma and death”, manifestations similar to syndrome AIDS. • In 1956 in central Africa, - “gay fever”. • In 1981 - first recognized Cases in New York, Los Angeles and San Francisco.
1981 - 1st report on AIDS – “morbidity and mortality” by USCDC . • 1982 - human T lymphotropic virus-I (HTLV-I) isolated in Japan. • 1983-HTLV-II isolated in US, (Miyoshi et.al) related to Asian money. • 1983 - first case of unexplained immuno -deficiency in children.
1983- Luc Montognier group at the Pasteur institute, Paris isolated retrovirus from west African patients with manifestation of AIDS. Named as (LAV) • 1984-Groopman isolated from saliva. • 1985 First test available • In 1986, International Committee on Taxonomy of virus proposed & was universally accepted as HIV
Status of HIV epidemic in India Maharashtra Manipur Andhra Pradesh Nagaland Highest- Tamil Nadu Karnataka High Prevalent states
HIV Prevalence Trend in India Prevalence 1998 3.5 m 1999 3.7 m 2000 3.86m 2001 3.97 m 2004 5.1 m 2006 2.45m Inference : infections are declining
` HIV-1 most common cause worldwide. Group M (major)- A to J Other groups - ‘O’ and ‘N’. Dominant subtype in western India - C
HIV-Infected T-Cell HIV Virus T-Cell HIV Infected T-Cell New HIV Virus
Earlier thought- HIV is labile virus. Now it has been confirmed that HIV can survive up to many hours/days out side the body. ---- Dr. Harold Jaffe • HIV Exposure and Infection • exposed one time & becomes infected • multipleexposures without infected
Window Period • Period of time after becoming infected when an HIV test is negative • 90 percent of cases test positive within three months of exposure • 10 percent of cases test positive within three to six months of exposure
Stage 1 - Primary • Short, flu-like illness - occurs one to six weeks after infection • no symptoms at all • Infected person can infect other people
Stage 2 - Asymptomatic • Lasts for an average of ten years • This stage is free from symptoms • There may be swollen glands • The level of HIV in the blood drops to very low levels • HIV antibodies are detectable in the blood
Stage 3 - Symptomatic • The symptoms are mild • The immune system deteriorates • Emergence of opportunistic infections and cancers
Stage 4 - HIV AIDS • The immune system weakens • The illnesses become more severe leading to an AIDS diagnosis
ARC COMPLEX • Not universally accepted • Composite of clinical signs and symptoms • Not a diagnostic stage • ARC includes presentation of- Chronic pyrexia Chronic diarrhea, Chronic weight loss and Some opportunistic infection like thrush
23659874515 Anonymous Anonymous Testing • No name is used • Unique identifying number • Results issued only to test recipient
Blood Detection Tests • Enzyme-Linked Immunosorbent Assay/Enzyme Immunoassay (ELISA/EIA). • Radio Immunoprecipitation Assay/Indirect Fluorescent Antibody Assay (RIA/IFA). • Polymerase Chain Reaction (PCR). 4. Western Blot test.
Urine Testing Urine Western Blot • As sensitive as testing blood • Safe way to screen for HIV • Can cause false positives in certain people at high risk for HIV
Oral Test. Orasure • FDA app.HIV antibody • Accurate as blood testing • Draws blood-derived fluids from the gum . • NOT A SALIVA TEST!
HIV in Body Fluids Average number of HIV particles in 1 ml Blood 18,000 Semen 11,000 Vaginal Fluid 7,000 Amniotic Fluid 4,000 Saliva 1
ORAL MANIFESTATIONS OF AIDS
Cervical Caries Associated with Xerostomia • Angular Cheilitis
PseudomembranousCandidiasis—Mild or Moderate severe form
Linear GingivalErythema Necrotizing Ulcerative Periodontitis
Aphthous Ulceration Neutropenic Ulcerations
Risk of Vertical Transmission • The probability that an HIV positive woman’s baby will become infected if no anti- retrovirals are administered to mother or child is as high -as 35%.
Virologic Tests Used in Infants • HIV DNA PCR • HIV culture • HIV RNA PCR • P24 Antigen
Immune Function in Children Total CD4 counts in normal infants are considerably higher than adults. Therefore, CD4 Percentage should be used to monitor disease Clinical Progression of HIV in children Average 70% Rapid 20% Long Term 10% AIDS Education and Training Centers National Resource Center,2003
Stage1 Asymptomatic Generalized Lymphadenopathy WHO Staging Stage 2 Chronic Diarrhea , Fever Recurrent Candidiasis Failure to Thrive/Weight Loss Recurrent Bacterial Infections Stage 3 Severe Failure to Thrive Encephalopathy Malignancy AIDS Defining Opportunistic Infection Progressive encephalopathy
Detection of Symptomatic HIV Suspected Symptomatic HIV Infection
Oral Thrush Parotitis
Herpes Zoster MolluscumContagiosum
Routine Care of HIV Infected Paediatric Patients • Monitor growth and development • Immunisation • Vitamin A supplementation • Co-trimoxazole prophylaxis • Counsel nutrition • Family support/ Health of Caregivers • Dental Care