Download
1 / 52
620 likes | 1.44k Views
Antipsychotic (Neuroleptic) Drugs . Psychosis. Psychosis is a thought disorder characterized by disturbances of reality and perception, impaired cognitive functioning, and inappropriate or diminished affect (mood). Psychosis denotes many mental disorders.

E N D
Psychosis • Psychosis is a thought disorder characterized by disturbances of reality and perception, impaired cognitive functioning, and inappropriate or diminished affect (mood). • Psychosis denotes many mental disorders. • Schizophrenia is a particular kind of psychosis characterized mainly by: • a clear sensorium • a marked thinking disturbance.
Schizophrenia • Pathogenesis is unknown. • Onset of schizophrenia is in the late teens early twenties. • Genetic predisposition -- Familial incidence. • Multiple genes are involved. • Afflicts 1% of the population worldwide.
Schizophrenia Positive Symptoms. • Symptoms that most individuals do not normally experience. • They include: • delusions • auditory hallucinations • thought disorder • are typically regarded as manifestations of psychosis.
Negative Symptoms. • considered to be the loss or absence of normal traits or abilities. • Include features such as: • flat or blunted affect and emotion • poverty of speech (alogia) • inability to experience pleasure (anhedonia) • lack of motivation (avolition) • These symptoms are progressive and non-responsive to medication.
Disorganization syndromeincludes: chaotic speech, thought, and behavior
Drugs currently used in the prevention of psychosis. • They have also been termed neuroleptics, because they suppress motor activity and emotionality. ** These drugs are not a cure ** • Schizophrenics must be treated with medications indefinitely, in as much as the disease in lifelong and it is preferable to prevent the psychotic episodes than to treat them.
Antipsychotic treatments SCHIZOPHRENIA IS FOR LIFE There is no remission
All currently available antipsychotic drugs that alleviate symptoms of schizophrenia decrease dopaminergic and/or serotonergic neurotransmission.
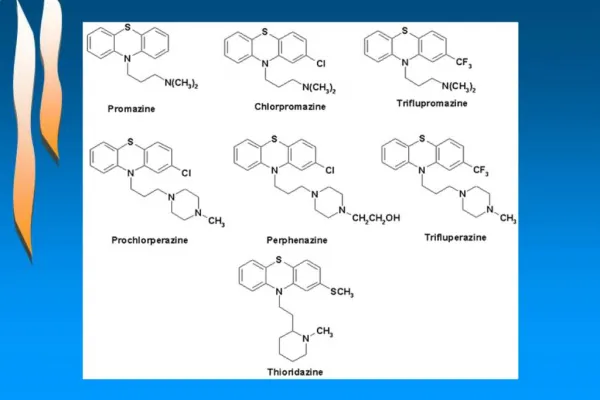
Classification • Typical (conventional) antipsychotic drugs: • Often subclassified according to their oral potency (high potency or low potency). • High-potency drugs • piperazine phenothiazines, e.g., fluphenazine • butyrophenones e.g., haloperidol • more likely to produce extrapyramidal reactions.
Low-potency drugs • aliphatic phenothiazines, e.g.,triflupromazine • piperidine phenothiazines, e.g., thioridazine • are less likely to produce acute extrapyramidal reactions • more likely to produce sedation and postural hypotension.
Atypical antipsychotic drugs • e.g., Clozapine, risperidone, olanzapine • have generally replaced the conventional drugs for initial treatment of first-episode patients. • Clozapine is reserved for treatment-resistant patients. • Other typical heterocyclic antipsychotic drugs • e.g., loxapine and molindone • intermediate potency • have no clear advantage over other conventional drugs.
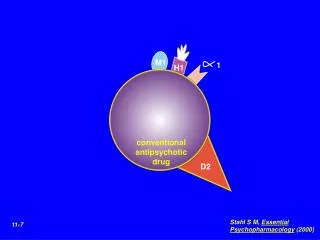
Mechanism of therapeutic action • The therapeutic action of the typical antipsychotic drugs is correlated best with antagonist activity at postjunctional dopamine D2-receptors, where dopamine normally inhibits adenylyl cyclase activity.
The therapeutic action of the atypical antipsychotic drugs is correlated with antagonist activity at both: • 5-HT2-receptors • Dopamine D2- or D4-receptors. • Aripiprazole is a partial agonist at dopamine D2-receptors • Aripiprazole and ziprasidone, also stimulates serotonin 5-HT1A-receptors.
The therapeutic action is best correlated with the actions of these drugs in the mesolimbic and mesocortical areas of the CNS.
Pharmacologic properties • Most of these drugs show little correlation between plasma levels and therapeutic action. Plasma levels are monitored primarily for compliance and toxicity. • Most antipsychotic drugs are highly lipophilic and have long half-lives (10—20 h). • They are metabolized by liver microsomal oxidation and conjugation.
Esterification of fluphenazine and haloperidol (fluphenazine decanoate, haloperidol decanoate) results in long-acting depot forms (2- to 3-week duration of action) that can be used to manage compliance issues. • Plasma esterases convert the parent compound to the active drug when the ester diffuses into the bloodstream.
Therapeutic uses • Schizophrenia • Their antipsychotic effects, including • decreasing the positive symptoms: symptoms of thought disorders, paranoid features, delusions, hostility, hallucinations • to a lesser degree decreasing the negative symptoms: • decreased withdrawal • apathy • blunted affect.
Atypical antipsychotic drugs, particularly clozapine, have a seemingly greater effect on negative symptoms than the conventional agents. • These drugs curb acute psychotic attacks and delay subsequent relapses.
Other selected therapeutic uses: • Acute mania in bipolar disorder • Atypical psychotic disorders (e.g., following surgery or myocardial infarction) • Depression with psychotic manifestations • Tourette's syndrome (haloperidol or pimozide), to suppress severe tics and vocalization
Severe nausea or vomiting: • Conventional antipsychotics have strong antiemetic activity due to dopamine D2-receptor blockade in the chemoreceptor trigger zone of the medulla. • Prochlorperazine: most commonly used • Promethazine
Adverse effects and contraindications • The adverse effects of antipsychotic agents are due to their antagonist actions at receptors • in the CNS • dopamine D2-receptors • histamine H1-receptors • (and possibly serotonin receptors) • in the periphery • muscarinic cholinoceptors • α-adrenoceptors
Central nervous system A. Extrapyramidal syndromes • These adverse effects are related to a dopamine-receptor blockade in the basal ganglia (and elsewhere in the CNS) that leads to an imbalance in dopamine and acetylcholine actions in the nigrostriatal pathway. • These effects are a major cause of noncompliance.
Extrapyramidal effects are: • most likely to occur with high-potency conventional antipsychotic drugs that have a high affinity for postjunctional dopamine D2-receptors in the basal ganglia. • occur with few atypical drugs like risperidone. • These effects can sometimes spontaneously remit.
Extrapyramidal syndromes include the following: • Acute dystonia: sustained muscle contractions cause twisting and repetitive movements or abnormal postures • This condition is often elicited during the first week of therapy. • Akathisia is the irresistible compulsion to be in motion. • This condition can develop as early as the first 2 weeks of treatment or as late as 60 days into therapy. • Parkinsonian-like syndrome • Parkinsonian-like syndrome is characterized by tremors, bradykinesia, rigidity, and other signs of parkinsonism. • This syndrome can develop from 5 days to weeks into treatment.
Tardive dyskinesia (10—20%) • CNS disorder characterized by: • twitching of the face and tongue • involuntary motor movements of the trunk and limbs • More likely with conventional antipsychotic agents. • Tardive dyskinesia generally occurs after months to years of drug exposure; it may be exacerbated or precipitated by the discontinuation of therapy.
Orofacial movements Dystonic posture
Tardive dyskinesia is often irreversible. • more likely to occur in the elderly or in institutionalized patients who receive long-term, high-dose therapy. • The only effective treatment for tardive dyskinesia is the discontinuation of treatment.
Neuroleptic malignant syndrome • Due to excessively rapid blockade of postsynaptic dopamine receptors. • This syndrome is characterized by: • altered blood pressure and heart rate. • muscle rigidity • diaphoresis • profound hyperthermia • myoglobinemia • This condition occurs, often explosively, in 1% of patients; it is associated with a 20% mortality rate.
This condition is treated by: • discontinuing drug therapy • initiating supportive measures, including the use of bromocriptine to overcome the dopamine receptor blockade • muscle relaxants such as dantrolene and diazepam to reduce muscle rigidity.
Sedation • More likely with low-potency antipsychotic agents and with the atypical agents, are due to a central histamine H1-receptor blockade. • These effects may be mild to severe. • The elderly are particularly at risk. • May be temporary
e. Confusional state with memory impairment. • This effect is likely with antipsychotic agents with pronounced antimuscarinic activity. • Seizures • Seizures are especially common with chlorpromazine and clozapine. • This effect is due to a lowering of the seizure threshold; antipsychotic drugs may precipitate or unmask epilepsy.
Autonomic Nervous system • α-Adrenoceptor blockade • More likely to occur with: • conventional low-potency • atypical antipsychotic agents. • Postural hypotension- phenothiazines when a person moves to a more vertical position: from sitting to standing or from lying down to sitting or standing. • Orthostatic hypotention – atypical drugs symptoms: dizziness, faintness or lightheadedness which appear only on standing, and which are caused by low blood pressure. • Failure to ejaculate -phenothiazines
Muscarinic cholinoceptor blockade • More common with: • conventional low-potency antipsychotic agents • atypical agent clozapine. • Muscarinic receptor blockade, atropine-like effects (dry mouth, constipation, urinary retention, and visual problems) • Elderly patients are more at risk • The effects may be temporary.
Endocrine and metabolic disturbances • Most likely with • most conventional antipsychotic agents • atypical agent risperidone • Due to dopamine (D2)-receptor antagonist activity in the pituitary, resulting in hyperprolactinemia.
DA HYPOTHALAMUS DA (-) PRL Anterior Pituitary PRL (+) BREAST
In women, these disturbances include: • galactorrhea • loss of libido • delayed ovulation and menstruation or amenorrhea. • In men, these disturbances include: • gynecomastia • impotence.
Weight gain, which is likely with: • most conventional • atypical antipsychotic agents, except aripiprazole and ziprasidone, may be due in part to histamine H1-receptor antagonist activity.
Other adverse effects • Withdrawal-like syndrome • Symptoms: nausea, vomiting, insomnia, and headache • in 30% of patients, especially those receiving low-potency antipsychotic drugs. • Symptoms may persist for up to 2 weeks. • Symptoms can be minimized with a tapered reduction of drug dosage.
Cardiac arrhythmias • More likely with thioridazine and ziprasidone, which • Can prolong the Q-T interval and lead to conduction block and sudden death.
Blood dyscrasias • rare, except in the case of clozapine, which may induce agranulocytosis (severe neutropenia) in up to 3% of patients and, therefore, is used only when other drug groups prove ineffective.
Cholestatic jaundice, which is caused primarily by chlorpromazine • Photosensitivity • The effect is specific to chlorpromazine • it includes dermatitis (5%), rash, sunburn, and pigmentation, and it may be irreversible. • Chlorpromazine and high-dose thioridazine also produce retinitis pigmentosa
Overdose. • rarely fatal, except when caused by thioridazine or mesoridazine (and possibly ziprasidone), which may result in drowsiness, agitation, coma, ventricular arrhythmias, heart block, or sudden death.
Drug Interactions • Additive effects with sedatives. • Additive effects with anticholinergics. • Additive effects with antihistaminergics. • Additive effects with -AR blocking drugs. • Additive effects with drugs with quinidine-like action (thioridazine).