Download
1 / 1
20 likes | 200 Views
Neuroleptic Malignant Syndrome Presenting To The Emergency Department Gregory Fenati, DO 1 , Micheal Neeki, DO,MS 2 1 Department of Emergency Medicine, Arrowhead Regional Medical Center, Colton, CA. INTRODUCTION

E N D
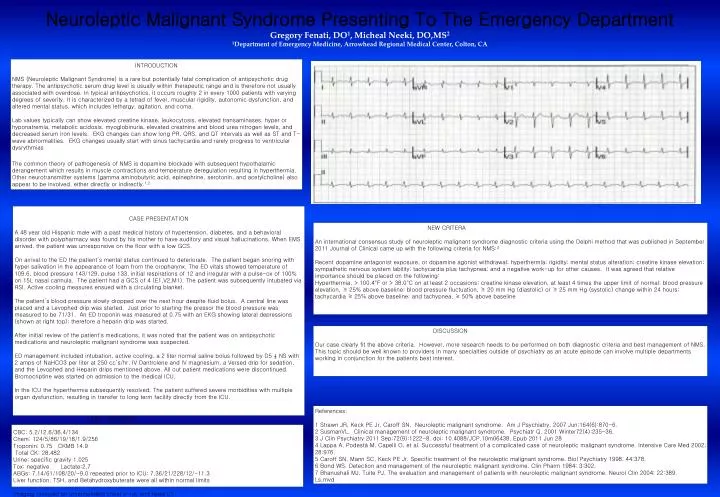
Neuroleptic Malignant Syndrome Presenting To The Emergency Department Gregory Fenati, DO1, Micheal Neeki, DO,MS2 1Department of Emergency Medicine, Arrowhead Regional Medical Center, Colton, CA INTRODUCTION NMS (Neuroleptic Malignant Syndrome) is a rare but potentially fatal complication of antipsychotic drug therapy. The antipsychotic serum drug level is usually within therapeutic range and is therefore not usually associated with overdose. In typical antipsychotics, it occurs roughly 2 in every 1000 patients with varying degrees of severity. It is characterized by a tetrad of fever, muscular rigidity, autonomic dysfunction, and altered mental status, which includes lethargy, agitation, and coma. Lab values typically can show elevated creatine kinase, leukocytosis, elevated transaminases, hyper or hyponatremia, metabolic acidosis, myoglobinuria, elevated creatnine and blood urea nitrogen levels, and decreased serum iron levels. EKG changes can show long PR, QRS, and QT intervals as well as ST and T-wave abnormalities. EKG changes usually start with sinus tachycardia and rarely progress to ventricular dysrythmias The common theory of pathogenesis of NMS is dopamine blockade with subsequent hypothalamic derangement which results in muscle contractions and temperature deregulation resulting in hyperthermia. Other neurotransmitter systems (gamma aminobutyric acid, epinephrine, serotonin, and acetylcholine) also appear to be involved, either directly or indirectly.1,2 1 2 3 A B CASE PRESENTATION A 48 year old Hispanic male with a past medical history of hypertension, diabetes, and a behavioral disorder with polypharmacy was found by his mother to have auditory and visual hallucinations. When EMS arrived, the patient was unresponsive on the floor with a low GCS. On arrival to the ED the patient’s mental status continued to deteriorate. The patient began snoring with hyper salivation in the appearance of foam from the oropharynx. The ED vitals showed temperature of 109.6, blood pressure 143/129, pulse 133, initial respirations of 12 and irregular with a pulse-ox of 100% on 15L nasal cannula. The patient had a GCS of 4 (E1,V2,M1). The patient was subsequently intubated via RSI. Active cooling measures ensued with a circulating blanket. The patient’s blood pressure slowly dropped over the next hour despite fluid bolus. A central line was placed and a Levophed drip was started. Just prior to starting the pressor the blood pressure was measured to be 71/31. An ED troponin was measured at 0.75 with an EKG showing lateral depressions (shown at right top); therefore a heparin drip was started. After initial review of the patient's medications, it was noted that the patient was on antipsychotic medications and neuroleptic malignant syndrome was suspected. ED management included intubation, active cooling, a 2 liter normal saline bolus followed by D5 ½ NS with 2 amps of NaHCO3 per liter at 250 cc’s/hr, IV Dantrolene and IV magnesium, a Versed drip for sedation, and the Levophed and Heparin drips mentioned above. All out patient medications were discontinued. Bromocriptine was started on admission to the medical ICU. In the ICU the hyperthermia subsequently resolved. The patient suffered severe morbidities with multiple organ dysfunction, resulting in transfer to long term facility directly from the ICU. NEW CRITERA An international consensus study of neuroleptic malignant syndrome diagnostic criteria using the Delphi method that was published in September 2011 Journal of Clinical came up with the following criteria for NMS:3 Recent dopamine antagonist exposure, or dopamine agonist withdrawal; hyperthermia; rigidity; mental status alteration; creatine kinase elevation; sympathetic nervous system lability; tachycardia plus tachypnea; and a negative work-up for other causes. It was agreed that relative importance should be placed on the following: Hyperthermia, > 100.4°F or > 38.0°C on at least 2 occasions; creatine kinase elevation, at least 4 times the upper limit of normal; blood pressure elevation, ≥ 25% above baseline; blood pressure fluctuation, ≥ 20 mm Hg (diastolic) or ≥ 25 mm Hg (systolic) change within 24 hours; tachycardia ≥ 25% above baseline; and tachypnea, ≥ 50% above baseline DISCUSSION Our case clearly fit the above criteria. However, more research needs to be performed on both diagnostic criteria and best management of NMS. This topic should be well known to providers in many specialties outside of psychiatry as an acute episode can involve multiple departments working in conjunction for the patients best interest. References: 1 Strawn JR, Keck PE Jr, Caroff SN. Neuroleptic malignant syndrome. Am J Psychiatry. 2007 Jun;164(6):870-6. 2 SusmanVL. Clinical management of neuroleptic malignant syndrome. Psychiatr Q. 2001 Winter72(4):235-36. 3 J Clin Psychiatry 2011 Sep;72(9):1222-8. doi: 10.4088/JCP.10m06438. Epub 2011 Jun 28 4 Lappa A, Podestà M, Capelli O, et al. Successful treatment of a complicated case of neuroleptic malignant syndrome. Intensive Care Med 2002; 28:976. 5 Caroff SN, Mann SC, Keck PE Jr. Specific treatment of the neuroleptic malignant syndrome. Biol Psychiatry 1998; 44:378. 6 Bond WS. Detection and management of the neuroleptic malignant syndrome. Clin Pharm 1984; 3:302. 7 Bhanushali MJ, Tuite PJ. The evaluation and management of patients with neuroleptic malignant syndrome. Neurol Clin 2004; 22:389. Ls,mvd LABS / IMMAGING CBC: 5.2/12.6/36.4/134 Chem: 124/5/86/19/18/1.9/256 Troponin: 0.75 CKMB 14.9 Total CK: 28,482 Urine: specific gravity 1.025 Tox: negative Lactate:2.7 ABGs: 7.14/61/108/20/-9.0 repeated prior to ICU: 7.36/21/228/12/-11.3 Liver function, TSH, and Betahydroxybuterate were all within normal limits Imaging revealed an unremarkable chest x-ray and head CT