Download
1 / 2
20 likes | 58 Views
Evaluate impact-u00a0Heavy menstrual bleeding ( HMB ) is one of the commonest reason for gynecological referral and consultations About 1 in 20 women aged 30-49 yrs see GP/ year for HMB or menstrual problems Menstrual disorders comprise u202812 % of all referral to gynecology service The guideline states that HMB has a major impact on a womens QOL and advises to ensure that any intervention should aim to improve this rather than focusing on blood loss<br>https://www.a4medicine.co.uk/heavy-menstrual-bleeding/<br>

E N D
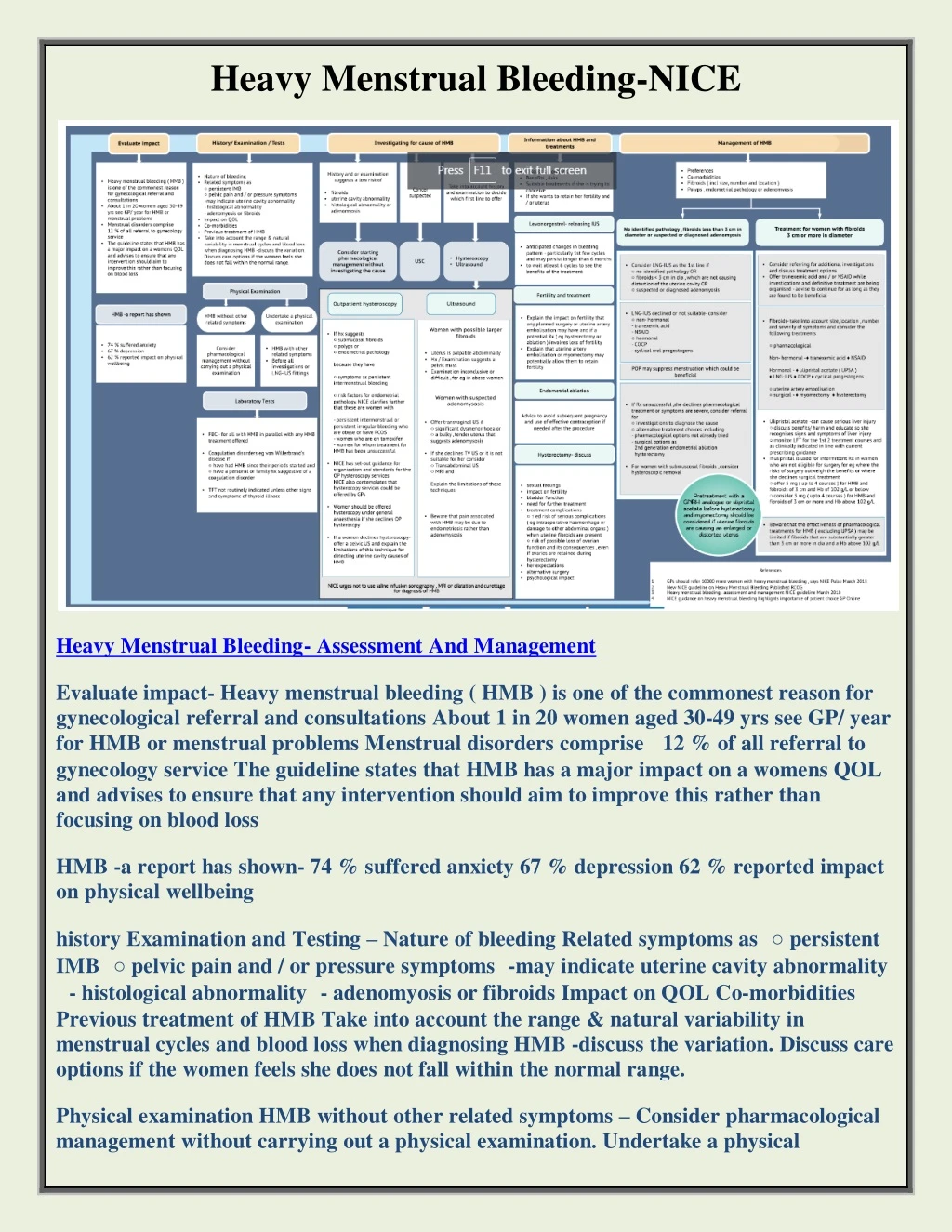
Heavy Menstrual Bleeding-NICE Heavy Menstrual Bleeding- Assessment And Management Evaluate impact- Heavy menstrual bleeding ( HMB ) is one of the commonest reason for gynecological referral and consultations About 1 in 20 women aged 30-49 yrs see GP/ year for HMB or menstrual problems Menstrual disorders comprise 12 % of all referral to gynecology service The guideline states that HMB has a major impact on a womens QOL and advises to ensure that any intervention should aim to improve this rather than focusing on blood loss HMB -a report has shown- 74 % suffered anxiety 67 % depression 62 % reported impact on physical wellbeing history Examination and Testing – Nature of bleeding Related symptoms as ○ persistent IMB ○ pelvic pain and / or pressure symptoms -may indicate uterine cavity abnormality - histological abnormality - adenomyosis or fibroids Impact on QOL Co-morbidities Previous treatment of HMB Take into account the range & natural variability in menstrual cycles and blood loss when diagnosing HMB -discuss the variation. Discuss care options if the women feels she does not fall within the normal range. Physical examination HMB without other related symptoms – Consider pharmacological management without carrying out a physical examination. Undertake a physical
examination-HMB with other related symptoms Before all investigations or LNG-IUS fittings Lab tests – FBC – for all with HMB in parallel with any HMB treatment offered Coagulation disorders eg von Willerbrand’s disease if ○ have had HMB since their periods started and ○ have a personal or family hx suggestive of a coagulation disorder TFT not routinely indicated unless other signs and symptoms of thyroid illness investigating the cause –History and or examination suggests a low risk of fibroids uterine cavity abnormality histological abnormality or adenomyosis. Consider starting pharmacological management without investigating the cause. Cancer suspected- USC. Take into account history and examination to decide which first line to offer. Outpatient hysteroscopy. If hx suggests ○ submucosal fibroids ○ polyps or ○ endometrial pathology because they have ○ symptoms as persistent intermenstrual bleeding for endometrial pathology. NICE clarifies further that these are women with persistent intermenstrual or persistent irregular bleeding who are obese or have PCOS - women who are on tamoxifen - women for whom treatment for HMB has been unsuccessful NICE has set-out guidance for organization and standards for the OP hysteroscopy services NICE also contemplates that hysterocopy services could be offered by GPs Women should be offered hysterocopy under general anesthesia if she declines OP hysteroscpy If a women declines hysteroscopy- offer a pelvic US and explain the limitations of this technique for detecting uterine cavity causes of HMB. ○ risk factors - ultrasound -women with possible larger fibroids Uterus is palpable abdominally Hx / Examination suggests a pelvic mass Examination inconclusive or difficult , for eg in obese women. Visit: https://www.a4medicine.co.uk/heavy-menstrual-bleeding/