Download
1 / 20
210 likes | 643 Views
By Dr Michael Tombros 18.3.2009. CG44 Heavy Menstrual Bleeding. Menstrual loss > 80mls per month Heavy Menstrual Bleeding (HMB) = excessive blood loss interfering with physical, emotional, social and material QOL. Definition of Menorrhagia. Menorrhagia.

E N D
By Dr Michael Tombros 18.3.2009 CG44 Heavy Menstrual Bleeding
Menstrual loss > 80mls per month Heavy Menstrual Bleeding (HMB) = excessive blood loss interfering with physical, emotional, social and material QOL Definition of Menorrhagia
Menorrhagia • Up to 30% complain of this but only half have menstrual loss > 80 mls • > 10 pads or tampons per day • Passage of clots
Assessment • History and pattern of bleeding • Pain • Contraceptive needs • Family history of bleeding tendencies • Drug history
Examination • Anaemia • Pelvic examination (chronic infection or endometriosis) • Adnexal tenderness • Endometrial polyps • Abdominal examination (pelvic masses/tenderness)
Investigation • FBC • Clotting screen • TFTs (not recommended by NICE 2007) • Cervical smear • Endocervical swabs • Pelvic +/- transvaginal USS • Biopsy if appropriate (endometrial CA, atypical hyperplasia): over 45, persistent intermenstrual bleeding, ineffective treatment
Differential • Physiological bleeding or dysfunctional uterine bleeding (50%) • Fibroids • Bicornuate uterus • Pelvic infection • Endometriosis • Endometrial polyps • IUCD • Endometrial carcinoma • Coagulopathy (eg Von Willebrand's)
Management • Pharmaceutical: hormonal or non-hormonal • Non-hysterectomy surgery: endometrial ablation in women with uterus no bigger than 10/40 pregnancy • Hysterectomy
Management • Very heavy bleeding: • Noresthisterone 10mg TDS • Reduce dose over 7-10 days • Check FBC • Refer gynae
Reasons to refer • Age > 40 • Uterus >10/40 • Intermenstrual or poistcoital bleeding • Pelvic pain between periods • Failed medical treatment • History of tamoxifen/unopposed oestrogens
If doesn't want hormones or does not require contraception • Mefanemic acid 500mg TDS (NSAID) – can also try ibuprofen and naproxen (indigestion, asthma, PUD) – preferred over tranexamic acid in dysmenorrhoea • Tranexamic acid 1g TDS (anti-fibrinolytic agent), SE diarrhoea, indigestion, headache • (starting on 1st day of period for days of heavy flow) • Use for 3 months if no improvement • Either continue indefinitely or REFER if not controlled/side effects + try other drug while waiting
Needs contraception also • Progestogen IUD or Long-acting progestogens (Levonogestrel-releasing intrauterine system): • Review in 6 months +/- REFER • Combined pill: • Review after 3 months +/- add mefanemic acid then review in 3 months +/- REFER • Progestogens
Has copper or non-hormonal IUD in place • Add tranexamic acid OR mefanemic acid • Change to Progestogen releasing IUS • If still unacceptable remove IUD and suggest alternative contraception • Side effects of hormonal IUS = irregular bleeding, breast tenderness, acne, headaches, amenorrhoea, uterine perforation
Progestogens • Prevent proliferation of endometrium • Oral luteal phase progestogens are ineffective in reducing blood flow eg. Femulen,Micronor, Microval, Neogest, Norgeston, Noriday • Intrauterine progestogens are effective • Long acting progestogens (im) • Norethisterone (oral) • Weight gain, headache, depression, PMS, acne, breast tenderness, amenorrhoea, bloating
Summary of Evidence (data from national collaborating centre for women's and children's health, 2007)
Pharamceutical Treatments according to NICE • 1st line = Levonorgestrel-releasing IUD • 2nd line = tranexamic acid, NSAIDS, combined oral contraceptive • 3rd line = oral progestogen (norethisterone) or injected progestogen • 'other' = Gn-RH analogue injection, S/E = menopausal symptoms (Stops oestrogen and progesterone production)
NICE do not recommend: • Luteal phase oral progestogens • Danazol • Etamsylate • Dilatation and Curettage
Investigations that are NOT recommended • Menstrual blood loss measurements • Serum ferritin • Female hormone testing • TFTs • Saline infusion USS • MRI • D and C
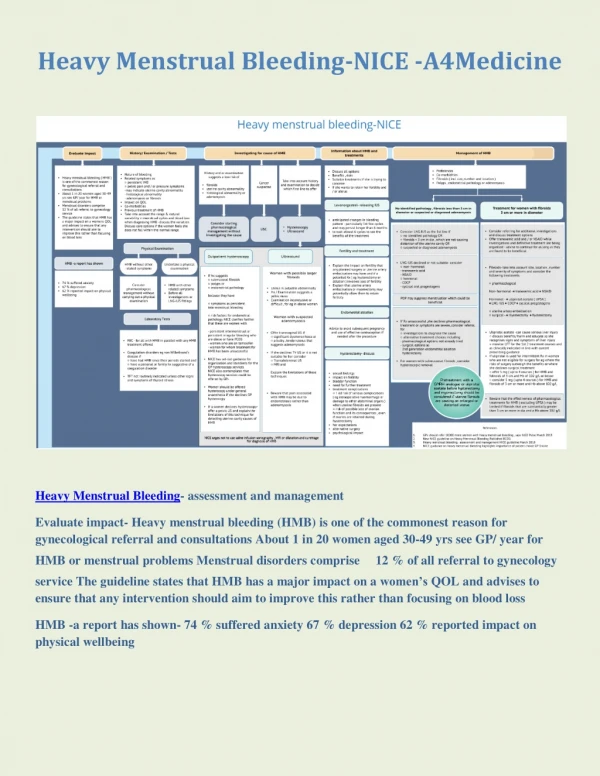
Summary • First line treatment is IUS (Mirena) if contraception needed or combined pill (second line) • If contraception not needed then: NSAID, tranexamic acid • 3rd line treatments = progestogens (noresthisterone or progestogen injection)