Download
1 / 33
350 likes | 720 Views
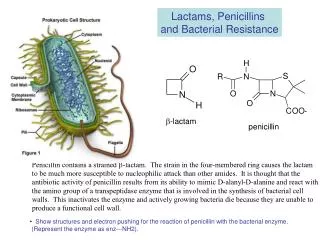
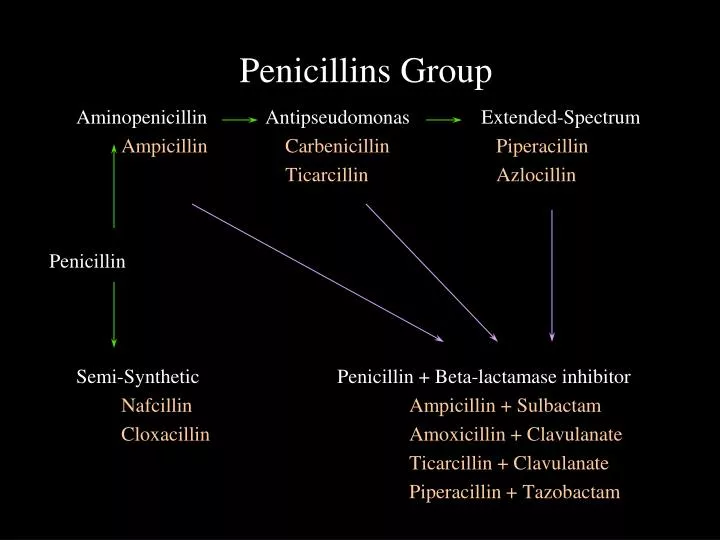
Penicillins Group. Aminopenicillin Antipseudomonas Extended-Spectrum Ampicillin Carbenicillin Piperacillin Ticarcillin Azlocillin Penicillin Semi-Synthetic Penicillin + Beta-lactamase inhibitor Nafcillin Ampicillin + Sulbactam

E N D
Penicillins Group Aminopenicillin Antipseudomonas Extended-Spectrum Ampicillin Carbenicillin Piperacillin Ticarcillin Azlocillin Penicillin Semi-Synthetic Penicillin + Beta-lactamase inhibitor Nafcillin Ampicillin + Sulbactam Cloxacillin Amoxicillin + Clavulanate Ticarcillin + Clavulanate Piperacillin + Tazobactam
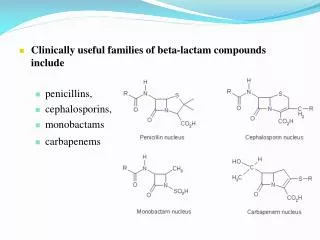
Cephalosporins Aminopenicillin Antipseudomonas Extended-Spectrum Gram -ve rod Pseudomonas Pseudomonas B.fragilis K.pneumoniae Penicillin Semi-Synthetic Staphylococci First generation (except H. influ)
First generation cephalosporins IV: Cefazolin PO: Cephalexin (Keflex) Cefadroxil
Cephalosporins Aminopenicillin Antipseudomonas Extended-Spectrum Gram -ve rod Pseudomonas Pseudomonas B.fragilis K.pneumoniae Penicillin Semi-Synthetic Staphylococci Second generation (include H. influ)
Second generation cephalosporins IV: Cefuroxime (Zinnat) PO: Cefuroxime (Zinnat), Cefaclor (Distraclor)
Cephalosporins Aminopenicillin Antipseudomonas Extended-Spectrum Gram -ve rod Pseudomonas Pseudomonas B.fragilis K.pneumoniae Penicillin Semi-Synthetic Third generation Staphylococci
Third generation cephalosporins • IV: Cefotaxime (Claforan), Ceftriaxone (Rocephin), Ceftazidime (Fortum), Cefoperazone (Cefobid) • PO: Cefixime (Cefspan), Cefdinir (Omnicef), Ceftibuten (Cedax), Cefodoxime proxetil (Banan)
Second generation (include H. influ) Cephalosporins Aminopenicillin Antipseudomonas Extended-Spectrum Gram -ve rod Pseudomonas Pseudomonas B.fragilis K.pneumoniae Penicillin Semi-Synthetic Third generation Staphylococci First generation (except H. influ)
Penicillin + Beta-Lactamase Inhibitors Active against Beta-lactamases producing organisms. Extension of the antimicrobial activity of the parent antibiotic. Except that neither ticarcillin nor piperacillin has been rended more active against Beta-Lactamases producing strains of Pseudomonas aeruginosa.
Drug interaction with AG Amphotericin BAdditive nephrotoxicity Cephalosporin/Enhanced nephrotoxicity &cephaloridineototoxicity CisplastinAdditive nephrotoxicity IndomethacinReduced renal clearance Loop diureticsEnhanced ototoxicity NeuromuscularEnhanced neuromuscular blocking agentsblockage
Vancomycin use MRSA CNS shunt infections Hemodialysis shunt infections Clostridium difficile ( Diarrhea, Colitis ) Meningitis caused by Gram-positive cocci, Diphtheroids Endocarditis ( Streptococcus viridans, MRSE ) Group D streptococci (enterococci) Group D non enterococci ( Streptococcus bovis )
NOT use Vancomycin Prophylaxis :Infections in ICU Surgical procedures General, Intra-abdominal Neurosurgical, Shunt, Graft Intravenous lines Antistaphylococcal coverage in febrile neutropenia Long-term ambulatory peritoneal dialysis
NOT use Vancomycin Therapy :MRSA colonization Enterococcal infections (esp. UTI) Gram +ve infections treatable by other antibiotics.
Imipenem Generally resistant MRSA Xanthomonas maltophilia Enterococcus faecium Pseudomonas cepacia Corynebacterium jeikeium Flavobacterium Clostridium difficile
NOT use Imipenem Alone in Rx serious Pseudomonasinfections (pneumonia) Community-acquired infection. Surgical prophylaxis. MRSA infection. Alone in Rx serious Enterococcalinfection (S. fecalis) Non-aeruginosa pseudomonal infections.
Lymphadenitis • S. aureus (MSSA or MRSA), group A strep • Empiric IV therapy • Oxacillin or • Cefazolin • For possible CA-MRSA • Clindamycin • Vancomycin
Bone and Joint Infections, Osteomyelitis, Infants and Children, Acute Infection • S. aureus, group A strep, rarely Kingella • For communities with over 5-10% MRSA • Start empirical therapy with clindamycin or vancomycin • Otherwise start oxacillin or cefazolin • Transition to oral therapy may be considered with cephalexin or dicloxacillin for MSSA once clinical improvement is documented and compliance ensured. • Total therapy (IV plus PO) for 4-6 wk
Arthritis – BacterialChildren • S. aureus, group A strep • MSSA • Oxacillin or cefazolin • Total therapy (IV plus PO) for 3 wk • MRSA • Clindamycin or vancomycin • As for osteomyelitis, transition to oral therapy may be considered once clinically improved
Pneumonia: Lobar or Segmental Consolidation – Community-Acquired • Pneumococcus (even if immunized), group A strep and S. aureus more likely in younger infants; Mycoplasma pneumonia pneumoniae and other atypical agents may cause lobar pneumonia in school-age children and adolescents • For hospitalized children: cefuroxime or ceftriaxone or cefotaxime; 10-14 d • For suspect mycoplasma and other atypical pneumonia pathogens: Add a macrolide • Oral outpatient therapy for less severe: Amoxicillin • For atypical pneumonia: Add agents as above
Pneumonia: Lobar or Segmental Consolidation – With Empyema • Group A strep • Penicillin G x 10 d • Pneumococcal • See above, Pneumonia: Lobar or segmental consolidation • S. aureus (consider CA-MRSA) • Vancomycin • For susceptible strains of MSSA: Oxacillin or cefazolin • MRSA: Clindamycin x > 21 d
Peritonitis - Primary • Pneumococcus • Ceftriaxone • Cefotaxime • If penicillin-susceptible • Penicillin G x 7-10 d
Peritonitis – Secondary to Bowel Perforation or Appendicitis • Enteric gram-negative bacilli, Bacteroides, Enterococcus • Meropenem • Imipenem • Clindamycin and ampicillin and gentamicin > 10 d
Abscess - Brain • Respiratory tract flora, skin flora, or bowel flora, depending on the pathogenesis of infection in a particular child • Until etiology established • Meropenem • Nafcillin and cefotaxime • Ceftriaxone and metronidazole • x 7-10 d after successful drainage • Longer therapy if no surgery • 3-6 wk
Empirical Therapy for Bacterial Meningitis • Cefotaxime • Ceftriaxone • Add vancomycin if gram-stain suggests pneumococcus
E. coli, Klebsiella • Extended-spectrum Β-lactamases • Resistance to cefotaxime, ceftriaxone, and ceftazidime
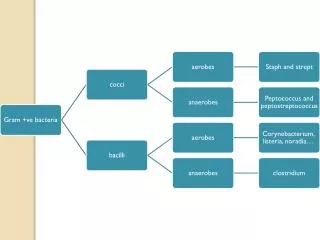
Gram negative: Drug resistance Enterobacter Serratia Klebsiella Acinetobacter Providentia/ Pseudomonas E.coli
CANDIDIASISEcology • Other clinically relevant species of Candida: • C. tropicalis – a cause of disseminated infection in compromised hosts • C. parapsilosis – second to C. albicans as a cause of endocarditis • C. glabrata – rare cause of endocarditis and disseminated infection in compromised hosts and catheter associated fungemia. Resistant to azoles • C. lusitaniae – can be a cause of fungemia and deep infection. Resistance to amphotericin B reported
COMMON CANDIDA SPECIES AND ANTIFUNGAL SUSCEPTIBILITY PATTERNS Continue on the next slide… (Treatment and Prevention of Fungal Infections: Focus on Candidemia, 2007.)
COMMON CANDIDAS SPECIES AND ANTIFUNGAL SUSCEPTIBILITY PATTERNS CONTINUE… (AMB=amphotericin B; FLU=fluconazole; ICU=intensive care unit; MIC=minimum inhibitory concentration)
Candida Species Flucon-azole Itracon-azole Voricon-azole Flucyto-sine AmBd Can-dins C. albicans S S S S S S C. tropicalis S S S S S S C.parapsilosis S S S S S S (to I?) C. glabrata S-DD to R S-DD to R S to I S S to I S C. krusei R S-DD to R S to I I to R S to I S C. lusitaniae S S S S S to R S General Patterns of Susceptibility of Candida Species S = Susceptible; I = Intermediate; S=DD = Susceptible dose-dependent; R = Resistant