Download
1 / 39
390 likes | 402 Views
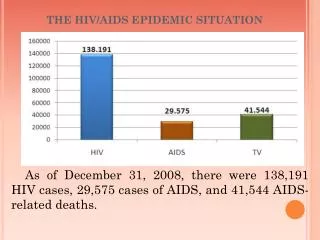
This update provides an overview of the HIV epidemic in Ontario, focusing on emerging situations among different populations. It discusses the methodologies and data sources used to estimate HIV incidence and prevalence, and presents findings related to men who have sex with men (MSM), injection drug users (IDU), individuals from HIV-endemic countries, and mother-infant transmission.

E N D
Epidemiologic Update on the HIV Epidemic in Ontario TheSituationintheYear2000 Robert S. Remis, MD, MPH, FRCPC Department of Public Health Sciences University of Toronto
Background • HIV epidemic in Ontario is unstable and dynamic • Monitoring trends in HIV transmission (incidence) and burden of HIV infection (prevalence) is critical to evaluate effectiveness of primary prevention and project the need for health and support services • Available data is biased and incomplete but triangulation allows obtaining plausible estimates for HIV incidence and prevalence Dr. Robert S. Remis Public Health Sciences, University of Toronto
Organization of presentation • Describe the databases and the methodologies used • Overview of HIV epidemic in Ontario • Focus on emerging situations • MSM • IDU • Persons from HIV-endemic countries • Mother-infant transmission Dr. Robert S. Remis Public Health Sciences, University of Toronto
Methods: Data sources • HIV diagnoses: First-time diagnoses at HIV Laboratory adjusted for unknown risk factors and previous HIV testing using data from Laboratory Enhancement Study • AIDS incidence: Cases diagnosed to December 1999 and reported by October 2000; • HIV-related mortality: Deaths to end 1997 adjusted for underascertainment • HIV-infected mothers and infants: Data reported to CPARG and analyzed by period of HIV diagnosis, infection status of infant and mother’s exposure category Dr. Robert S. Remis Public Health Sciences, University of Toronto
Methods: Data analysis • HIV model • HIV infection: incidence, cumulative incidence and prevalence • HIV diagnosis: incidence, cumulative incidence and prevalence • AIDS: incidence, cumulative incidence and prevalence • HIV-related mortality: incidence and cumulative incidence • Model values adjusted to fit available data on HIV diagnoses, reported AIDS cases and AIDS deaths and results from back-calculations Dr. Robert S. Remis Public Health Sciences, University of Toronto
Methods: Data analysis • HIV incidence from repeat testers • Results linked within HIV Laboratory database using name, sex, date of birth, previous test history to identify repeat testers • HIV incidence calculated by exposure category, age and health region using method of Kitayaporn • HIV incidence from detuned assay • HIV-positive sera tested using Abbott EIA assay rendered less sensitive to detect recent HIV infection (< 129 days) • HIV incidence = # discordant sera / (# tested x 129/365) Dr. Robert S. Remis Public Health Sciences, University of Toronto
Number of first-time HIV diagnoses by sexand proportion female, 1985–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
First-time HIV-positive diagnoses among males, n=17,878, HIV Laboratory, 1985–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
First-time HIV-positive diagnoses among females n=2,464,HIV Laboratory, 1985–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Reported AIDS cases among MSM, Ontario, 1981–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Reported AIDS cases by exposure category, Ontario, 1981–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
HIV incidence among MSM repeat testers, with 95% CLs, 1992-99 (28,103 PY) Source: Polaris Seroconversion Study
HIV incidence among MSM repeat testersby age group, 1992-99 Source: Polaris Seroconversion Study
HIV incidence among MSM repeat testers by health region, 1992-99 Source: Polaris Seroconversion Study
HIV incidence from detuned assay among MSM by health region, October 1999–June 2000 Source: Laboratory Enhancement Study
HIV incidence from detuned assay among MSM by age group, October 1999–June 2000 Source: Laboratory Enhancement Study
Modeled HIV incidence among MSMOntario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled HIV prevalence among MSM Ontario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled MSM population at risk, HIV prevalence and incidence by health region, Ontario, 1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
HIV incidence among IDU repeat testers with 95% CLs, 1992-99 (26,271 PY) Source: Polaris Seroconversion Study
HIV incidence among IDU repeat testers by health region, 1992-99 Source: Polaris Seroconversion Study
HIV Incidence from detuned assay among IDU by health region, October 1999–June 2000 Source: Laboratory Enhancement Study
Modeled HIV incidence among IDUsOntario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled HIV prevalence among IDUsOntario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled IDU population at risk, HIV prevalence and incidence by health region (aggregated), Ontario, December 1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
HIV incidence from detuned assay among MSM-IDU by health region,October 1999–June 2000 Source: Laboratory Enhancement Study
Modeled HIV prevalence among MSM-IDU by health region,1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled HIV incidence among persons from HIV-endemic regions, Ontario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled HIV prevalence among personsfrom HIV-endemic regions, Ontario, 1977–1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Modeled persons born in HIV-endemic countries, HIV prevalence and incidence by health regionOntario, 1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
HIV incidence among high risk versuslow risk heterosexual repeat testers Source: Polaris Seroconversion Study
Modeled HIV prevalence among heterosexuals by health region and sex,1999 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Proportion of HIV-infected infants by period of birth and exposure category of mother Ontario, 1984–1999 Source: Dr Susan King, CPARG
Number of HIV-positive mothers by antiretroviral prophylaxis and HIV status of infant, Ontario, July 1994-December 1999 Source: Dr Susan King, CPARG
HIV testing among pregnant women receiving prenatal care, Ontario, January 1999 to June 2000 Dr. Robert S. Remis Public Health Sciences, University of Toronto
Limitations • Populations at risk (especially MSM, IDU) are not well characterized (e.g. size, regional variations) • Adjustments for HIV diagnoses, AIDS cases and HIV-related mortality subject to uncertainty • Data on HIV incidence is limited and biased (likely overestimates); • However, these have been taken into account in HIV model Dr. Robert S. Remis Public Health Sciences, University of Toronto
Conclusions • HIV epidemic in Ontario is not yet under control • Good news: AIDS incidence and mortality have decreased • However . . . . . • Overall, HIV prevalence increased by 22% (16,480 to 20,050) and annual incidence by 50% (1,200 to 1,790) since 1996 • Increase in incidence among MSM: 80% (540 to 970) • MSM: preventive intervention efforts need to be systematically reviewed, reassessed and reinforced • HIV-endemic: prevention objectives and guidelines need to be developed and programs conceived, funded and implemented • Mother-infant: invest in education of physicians and women Dr. Robert S. Remis Public Health Sciences, University of Toronto
Conclusions • Limitations in available data limit precision of HIV incidence estimates; good studies are lacking • Cohort studies among MSM and IDU would be invaluable • HIV prevalence studies with correlates of infection • Prevention research: An idea whose time has come? Dr. Robert S. Remis Public Health Sciences, University of Toronto
Acknowledgements • Frank McGee, Coordinator, AIDS Bureau, Ontario Ministry of Health and Long Term Care (MOHLTC) • Carol Major and Carol Swantee, HIV Laboratory, MOHLTC • Liviana Calzavara, Ann Burchell and Polaris coinvestigators • Elaine P. Whittingham, University of Toronto • Susan King, Hospital for Sick Children • Evelyn Wallace and Lorraine Schiedel, Public Health Branch, MOHLTC • Ontario HIV Treatment Network (OHTN) • Instructional Media Centre, Laboratory Services,MOHLTC