Download
1 / 53
530 likes | 638 Views
Reuse of Data Coded with High-Quality Terminologies: Practical Examples from Patient Care Settings. James J. Cimino, M.D. Department of Biomedical Informatics Columbia University College of Physicians and Surgeons. Case Presentation.

E N D
Reuse of Data Coded with High-Quality Terminologies: Practical Examples from Patient Care Settings James J. Cimino, M.D. Department of Biomedical Informatics Columbia University College of Physicians and Surgeons
Case Presentation The patient is a 50 year old, Native American female who present to the emergency room with the chief complaint of cough and chest pain. The patient reports that she has had a productive cough for three days but that chest pain developed one hour ago. She gives a history of hypertension and states that she was getting a "capsule, half green, half blue-green" from her private doctor. She also reports that she was treated in the past for tuberculosis while she was pregnant, but doesn't remember what she was treated with or for how long. She reports that she was at another hospital on the other side of town, where she had a liver biopsy. She reports that she thinks the diagnosis was Hepatitis C. The patient reports an allergy to Bufferin. Physical examination revealed a well-developed, well-nourished female in moderate respiratory distress. Vital signs showed a pulse of 90, a respiratory rate of 22, an oral temperature of 100.3, and a blood pressure of 150/100. Examination revealed rales and rhonchi in the left upper chest. Abdominal exam revealed a tender, palpable liver edge. Labs: Chem7 (serum): Glucose 100 (70-105) Chem7 (plasma): Glucose 150 (75-110) CBC: Hgb 15 (12.0-15.8), Hct 45 (42.4-48.0), WBC 11,000 (3,540-9,060), Plate. 145K (165-415K) A fingerstick blood sugar was 80 Urinalysis showed protein of 1+ and glucose of 0 A blood culture was positive for methicillin-resistant Staphylococcus aureus (MRSA) ECG - Sinus Rhythm, 74BPM, Axis -30 degrees, ST segment 2mm elevated and T-waves down in leads I, L, V5 and V6 Chest X-ray Left upper lobe infiltrate, left ventricular hypertrophy The patient was admitted to the hospital, started on antibiotics and aspirin. A medical student reviewing the case is concerned about the risk of MRSA in patients with pneumonia and a recent myocardial infarction. She decides to do a literature search.
Case Presentation The patient is a 50 year old, Native American female who present to the emergency room with the chief complaint of cough and chest pain. The patient reports that she has had a productive cough for three days but that chest pain developed one hour ago. She gives a history of hypertension and states that she was getting a "capsule, half green, half blue-green" from her private doctor. She also reports that she was treated in the past for tuberculosis while she was pregnant, but doesn't remember what she was treated with or for how long. She reports that she was at another hospital on the other side of town, where she had a liver biopsy. She reports that she thinks the diagnosis was Hepatitis C. The patient reports an allergy to Bufferin. Physical examination revealed a well-developed, well-nourished female in moderate respiratory distress. Vital signs showed a pulse of 90, a respiratory rate of 22, an oral temperature of 100.3, and a blood pressure of 150/100. Examination revealed rales and rhonchi in the left upper chest. Abdominal exam revealed a tender, palpable liver edge. Labs: Chem7 (serum): Glucose 100 (70-105) Chem7 (plasma): Glucose 150 (75-110) CBC: Hgb 15 (12.0-15.8), Hct 45 (42.4-48.0), WBC 11,000 (3,540-9,060), Plate. 145K (165-415K) A fingerstick blood sugar was 80 Urinalysis showed protein of 1+ and glucose of 0 A blood culture was positive for methicillin-resistant Staphylococcus aureus (MRSA) ECG - Sinus Rhythm, 74BPM, Axis -30 degrees, ST segment 2mm elevated and T-waves down in leads I, L, V5 and V6 Chest X-ray Left upper lobe infiltrate, left ventricular hypertrophy The patient was admitted to the hospital, started on antibiotics and aspirin. A medical student reviewing the case is concerned about the risk of MRSA in patients with pneumonia and a recent myocardial infarction. She decides to do a literature search.
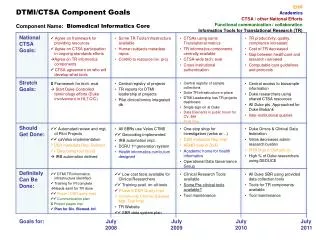
Use and Reuse of Clinical Data a) Automate the admission of the patient to a bed b) Summarize the patient’s blood sugar tests, including serum, plasma and fingerstick (but not urine) c) Use patient history to help with automated reminders d) Aggregate the patient’s data for quality assurance e) Use patient history to prevent adverse drug reactions f) Use the laboratory test results for automated diagnosis g) Use the patient’s data to automate information retrieval h) Aggregate the patient’s data for epidemiologic studies
Electronic Medical Record Admission Discharge Transfer System “Put the patient in Room 5, Bed B…” Automate the admission of the patient to a bed “Patient is an 50 year old, Native American female…”
Automate the admission of the patient to a bed But: how does the computer know that the patient is female? The record could say: “female” “Female” “FEMALE” “F” “Woman” “Girl”
Automate the admission of the patient to a bed • Data element - gender • Controlled terminology: • Male • Female • Unknown (don’t know) • Unknown (can’t tell) • Representation: • M,F,U1,U2 • 0,1,2,3 • What about other values? • Genotypic • Phenotypic • Administrative
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity
7 6 5 4 3 2 1 21 22 23 24 25 26 27 28 29 Information Form and Reuse
Summarize patient’s blood sugar tests, including serum, plasma and fingerstick (but not urine)
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity • Data model has terms too
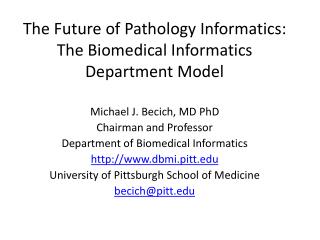
Medical Logic Modules Clinical Database Alerts & Reminders Database Monitor Results Review Database Interface Administrative Medical Entities Dictionary (MED) Research Reformatter Reformatter Reformatter . . . . . . Radiology Discharge Summaries Laboratory New York Presbyterian HospitalClinical Information Systems Architecture
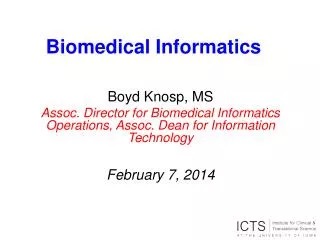
Substance Laboratory Specimen Event Chemical Anatomic Substance Plasma Specimen Diagnostic Procedure Substance Sampled Plasma Laboratory Test Laboratory Procedure Has Specimen Carbohydrate Bioactive Substance Part of Glucose Substance Measured MED Structure Medical Entity CHEM-7 Plasma Glucose Test
The MED Today • Concept-based (101,130) • Multiple hierarchy (150,480) • Synonyms (250,000) • Translations (180,000) • Semantic links (180,000) • Attributes (240,000)
Lab Test Chem20 Display Intravascular Glucose Test Using the MED for Summary Reporting Lab Display Fingerstick Glucose Test Serum Glucose Test Plasma Glucose Test
Summarize patient’s blood sugar tests, including serum, plasma and fingerstick (but not urine) DOP Summary
Summarize patient’s blood sugar tests, including serum, plasma and fingerstick (but not urine) WebCIS Summary
Summarize patient’s blood sugar tests, including serum, plasma and fingerstick (but not urine) Eclipsys Summary
Use patient history for automated reminders 489 Tuberculosis Codes in ICD9-CM 010. PRIMARY TB INFECTION* 010.0 PRIMARY TB COMPLEX* 010.00 PRIM TB COMPLEX-UNSPEC 010.01 PRIM TB COMPLEX-NO EXAM 010.02 PRIM TB COMPLEX-EXM UNKN 010.03 PRIM TB COMPLEX-MICRO DX 010.04 PRIM TB COMPLEX-CULT DX 010.05 PRIM TB COMPLEX-HISTO DX 010.06 PRIM TB COMPLEX-OTH TEST 011. PULMONARY TUBERCULOSIS* 012. OTHER RESPIRATORY TB* 013. CNS TUBERCULOSIS* 014. INTESTINAL TB* 015. TB OF BONE AND JOINT* 016. GENITOURINARY TB* 017. TUBERCULOSIS NEC* 018. MILIARY TUBERCULOSIS* 010.1 PRIMARY TB PLEURISY* 010.8 PRIM PROGRESSIVE TB NEC* 010.9 PRIMARY TB INFECTION NOS*
Use patient history for automated reminders More Tuberculosis in ICD9-CM 137. LATE EFFECT TUBERCULOSIS* 137.0 LATE EFFECT TB, RESP/NOS 137.1 LATE EFFECT CNS TB 137.2 LATE EFFECT GU TB 137.3 LATE EFF BONE & JOINT TB 137.4 LATE EFFECT TB NEC 647. INFECTIVE DIS IN PREG* 647.3 TUBERCULOSIS IN PREG* 647.30 TB IN PREG-UNSPECIFIED 647.31 TUBERCULOSIS-DELIVERED 647.32 TUBERCULOSIS-DELIV W P/P 647.33 TUBERCULOSIS-ANTEPARTUM 647.34 TUBERCULOSIS-POSTPARTUM
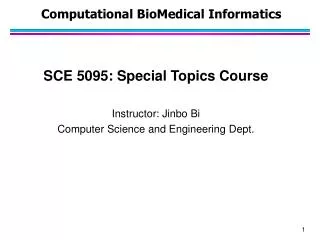
Infective Disease in Pregnancy (647) Primary TB (010) Pulmonary TB (011) Other Resp TB (012) Late Effect TB (137) TB in Preg (647.3) Primary TB Complex 010.0 Primary TB Pleurisy 010.1 Primary TB Complex No Exam 010.01 Primary TB Pleurisy No Exam 010.11 Primary TB Pleurisy Uspec 010.10 Primary TB Complex Uspec 010.00 Use patient history for automated reminders Tuberculosis Infection
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity • Data model has terms too • Multiple hierarchies
Reuse the patient’s data for quality assurance select patient_id , time = primary_time from visit2004_diagnosis where diagnosis_code = 2618 and b.primary_time between '01/01/2000' and '01/01/2005' and b.comp_code = 28144
Use patient history to prevent drug reactions has-ingredient Aspirin Preparations Method 1: Write a rule to check for each reaction Method 2: Include allergy codes for each medication Method 3: Include definitional information and infer Aspirin Bufferin Enteric-Coated Aspirin IF allergic drug [X] has ingredient [Y] AND ordered drug [Z] has ingredient [Y] THEN send alert
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity • Data model has terms too • Multiple hierarchies • Include definitional knowledge
Use test results for automated diagnosis Serum Specimen Abnormalities of Serum Potassium Potassium Serum Serum Potassium Test Hypokalemia
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity • Data model has terms too • Multiple hierarchies • Include definitional knowledge • Support automated translation
Use data for automated information retrieval Clinical Data Injectable Gentamicin Serum Gentamicin Level Has ingredient Substance Measured Gentamicin Decision Rule Measures Sensitivity Etiology Gentamicn Sensitivity Test Gentamicin Toxicity Drug Information Expert System
Reuse the patient’s data for epidemiologic studies 1995 1996
Requirements for High-Quality Terminology • Synonymy (not redundancy) • Multiple levels of granularity • Data model has terms too • Multiple hierarchies • Include definitional knowledge • Support automated translation • Avoid “Not Elsewhere Classified” (NEC)
Reuse the patient’s data for epidemiologic studies NEC • Can never have a formal definition • Terminology changes induce semantic drift
Viral Hepatitis Hepatitis A Hepatitis B Hepatitis C Hepatitis E Accommodating NEC
Accommodating NEC Viral Hepatitis Hepatitis A Hepatitis B Hepatitis, NEC Hepatitis E Hepatitis C
Hepatitis, NEC Hepatitis, NEC Accommodating NEC Viral Hepatitis Hepatitis A Retired Hepatitis B Hepatitis C Hepatitis E